
Volume 14 Issue 2 *Corresponding author mauraccrodrigues@gmail.com Submitted 23 May 2026 Accepted 20 Jun 2026 Published 12 Jul 2026 Citation RODRIGUES, M. C. C. et al. Interdisciplinary outpatient follow-up of high-risk newborns: experience report of a decade of an extension project at a university hospital in the Metropolitan Region of Rio de Janeiro. Coleção Estudos Cariocas, v. 14, n. 2, 2026.
DOI: 10.71256/19847203.14.2.234.2026 The article was originally submitted in PORTUGUESE. Translations into other languages were reviewed and validated by the authors and the editorial team. Nevertheless, for the most accurate representation of the subject matter, readers are encouraged to consult the article in its original language.


| Interdisciplinary outpatient follow-up of high-risk newborns: experience report of a decade of an extension project at a university hospital in the Metropolitan Region of Rio de Janeiro Seguimento ambulatorial interdisciplinar de recém-nascidos de alto risco: relato de experiência de uma década de um projeto extensionista em hospital universitário da Região Metropolitana do Rio de Janeiro Seguimiento ambulatorio interdisciplinario de recién nacidos de alto riesgo: relato de experiencia de una década de un proyecto extensionista en hospital universitario de la Región Metropolitana de Rio de Janeiro Maura Calixto Cecherelli de Rodrigues1, Alice Valente da Silva2, Cirlene de Lima Marinho3, Daiana Evangelista La Macchia4, Edneusa Oliveira Flor5 e Elaine Rego Menezes6, Eloá Gonçalves de Oliveira Campos7, Gloria Maria Bastos da Silva Bacelar8, João Mario Pereira da Silva9, Lucía de la Candelaria Arenas Viera10, Maria Aparecida Thiengo11, Simone Augusta Ribas12 1Universidade do Estado do Rio de Janeiro/Faculdade de Ciências Médicas/Departamento de Pediatria, ORCID 0000-0001-5711-1949, mauraccrodrigues@gmail.com 2Hospital Universitário Pedro Ernesto, ORCID 0000-0001-6792-9218, alicevalente@bol.com.br 3Hospital Universitário Pedro Ernesto, ORCID 0000-0001-5500-9684, cmarinho.uerj@gmail.com 4Hospital Universitário Pedro Ernesto, ORCID 0000-0003-2703-393X, daiana.evangelista@gmail.com 5Hospital Universitário Pedro Ernesto, ORCID 0000-0002-9760-0250, edneusa.neo@gmail.com 6Hospital Universitário Pedro Ernesto, ORCID 0000-0002-0164-3089, elaine.menez@gmail.com 7Hospital Universitário Pedro Ernesto, ORCID 0009-0004-1404-1169, elo.oliveirarj@gmail.com 8Hospital Universitário Pedro Ernesto, ORCID 0009-0004-6353-8235, gloria_bacelar@uol.com.br 9UERJ, Faculdade de Ciências Médicas, ORCID 0009-0002-0697-9013, jmjoaomario68@gmail.com 10Universidade do Estado do Rio de Janeiro, ORCID 0009-0001-2054-7367, arenas.lucia@gmail.com 11Hospital Universitário Pedro Ernesto, ORCID 0009-0007-3550-4099, m.thiengo@gmail.com 12Universidade Federal do Estado do Rio de Janeiro, ORCID 0000-0002-3947-9800, simone.ribas@unirio.br
Abstract Newborns discharged from Neonatal Units are a population vulnerable to neurodevelopmental disorders and other morbidities. This report describes the experience of the Extension Project Outpatient Follow-up of the High-Risk Newborn (SARAR), developed at a university hospital in the Metropolitan Region of RJ. The project promotes interprofessional and interdisciplinary follow-up, integrating care, teaching and research, and uses standardized instruments for developmental assessment, family-centered care and health education actions. The experience demonstrates the relevance of follow-up outpatient clinics in the early detection of health problems, timely intervention and qualification of academic training and maternal-child care. Keywords: high-risk newborn; outpatient follow-up; neurodevelopment. Resumo Os recém-nascidos egressos de Unidades de Terapia Neonatal são uma população vulnerável a alterações do neurodesenvolvimento e outras morbidades. Este relato descreve a experiência do Projeto de Extensão Seguimento Ambulatorial do Recém-Nascido de Alto Risco (SARAR), desenvolvido em um hospital universitário da Região Metropolitana do RJ. O projeto promove acompanhamento interprofissional e interdisciplinar, integrando assistência, ensino e pesquisa, e usa instrumentos padronizados de avaliação do desenvolvimento, cuidados centrados na família e ações de educação em saúde. A experiência demonstra a relevância dos ambulatórios de seguimento na detecção precoce de agravos, intervenção oportuna e qualificação da formação acadêmica e assistência materno-infantil. Palavras-chave: recém-nascido de alto risco; seguimento ambulatorial; neurodesenvolvimento. Resumen Los recién nacidos egresados de Unidades de Terapia Neonatal son una población vulnerable a alteraciones del neurodesarrollo y otras morbilidades. Este relato describe la experiencia del Proyecto de Extensión Seguimiento Ambulatorial del Recém-Nascido de Alto Risco (SARAR), desarrollado en un hospital universitario de la Región Metropolitana de RJ. El proyecto promueve acompañamiento interprofesional e interdisciplinario, integrando asistencia, enseñanza e investigación, y utiliza instrumentos estandarizados de evaluación del desarrollo, cuidados centrados en la familia y acciones de educación en salud. La experiencia demuestra la relevancia de los ambulatorios de seguimiento en la detección precoz de afecciones, intervención oportuna y calificación de la formación académica y la asistencia materno-infantil. Palabras clave: recién nacido de alto riesgo; seguimiento ambulatorio; neurodesarrollo. |
1 Introduction
Prematurity remains an important public health problem and ranks among the main causes of neonatal morbidity and mortality worldwide. In Brazil, the prevalence of premature births reached 11.9% in 2025, a percentage similar to that observed in the state of Rio de Janeiro (Brasil, 2025), reflecting the magnitude of the care, social and economic impact related to specialized neonatal care.
Technological advances in the neonatal field have enabled the survival of increasingly immature newborns (NB) with complex clinical conditions, especially those from Neonatal Intensive Care Units (NICU) (Howson et al., 2013). However, the reduction in neonatal mortality has not been accompanied by a proportional decline in associated neurological morbidities (Ferreira et al., 2020). Premature neonates, very low birth weight (< 1,500 g) and those affected by severe perinatal conditions, such as hypoxic-ischemic encephalopathy, sepsis and peri-intraventricular hemorrhage, constitute a population at high biological risk for the development of motor, cognitive, sensory and behavioral dysfunctions (Brasil, 2014; Darrah; Piper; Watt, 2008; Novak et al., 2017). Many of these disorders present subclinical phenotypes in the first months, manifesting themselves late during child development (Ferreira et al., 2020; Novak et al., 2017).
Similarly, and with possible concerning future negative impacts, neonates with perinatal asphyxia, i.e., those who suffered hypoxic-ischemic injury with systemic repercussions and especially to the developing brain, are at greater risk of developing delays and/or changes in their neurodevelopment and presenting clinical morbidities (Dias; Rodrigues; Duarte, 2024; Oliveira et al, 2024).
Given the complexity of this high-risk population, the structuring of longitudinal outpatient follow-up emerges as an imperative guideline in the continuity of perinatal care, enabling systematic monitoring of somatic growth and neurodevelopment, as well as screening and timely therapeutic intervention (Brasil, 2014). Beyond the management of acute clinical instabilities, prematurity and high-risk neonatal syndromes entail persistent deleterious impacts, increasing the prevalence of learning and language disorders, Attention Deficit Hyperactivity Disorder (ADHD), signs of Autism Spectrum Disorder and other mental health disorders and global functioning of the individual. Such outcomes require a multiprofessional, structured, prolonged clinical-therapeutic approach focused on the patient-family dyad (Ferreira et al., 2020).
The implementation and longitudinal retention of this assistance become, however, substantially challenging in metropolises characterized by deep socio-spatial inequalities and structural obstacles. In the context of Rio de Janeiro and its Metropolitan Region, intense socioeconomic vulnerabilities, urban mobility barriers and the systemic fragmentation of the health services network impose multiple obstacles to comprehensive maternal-child care (Bortz et al., 2015; Hone et al., 2023). Such deleterious factors may compromise the continuity of follow-up after discharge from the Neonatal Intensive Care Unit (NICU), exacerbating the risk of outpatient dropout and late diagnosis of developmental deviations (Vohr et al., 2009).
Given the demands of this complex care network, university hospitals assume a strategic position by organically integrating high-complexity care, teaching and translational research (Feuerwerker; Cecílio, 2007). The design and execution of interdisciplinary outpatient follow-up models in these settings allow not only the technical qualification of care offered to the high-risk pediatric population, but also the consolidation of academic training and the generation of scientific evidence aligned with the operational needs of the Unified Health System (SUS) (Peduzzi et al., 2013).
The Extension Project Outpatient Follow-up of the High-Risk Newborn (SARAR), operationalized since 2014 at a reference university hospital located in the North Zone of Rio de Janeiro, fits into this panorama as a vital strategy for longitudinal care aimed at neonates discharged from the NICU in an extensionist action model, that is, interprofessional, interdisciplinary and dialogically interactive. Structured on the inseparability of care, teaching, research and extension, the initiative proposes the holistic follow-up of the child and their family nucleus. The primary scope of the project falls on the early detection and intervention of neurodevelopmental and clinical morbidities, unique to this population, thus contributing to the promotion of Health and Well-being, the 3rd Sustainable Development Goal defined by the UN 2030 Agenda, and given the greater socioeconomic and health vulnerability, favoring Goal 10 of the 2030 Agenda, Reduction of Inequalities (Nações Unidas Brasil, 2015).
2 Objective
To report the experience of implementation and consolidation of a university extension project aimed at interdisciplinary outpatient follow-up of high-risk newborns, highlighting organization, functioning, care strategies, impacts on academic training and on health care and social development, and challenges related to the continuity of follow-up in the context of the Unified Health System.
3 Development of the Experience
The Extension Project Outpatient Follow-up of the High-Risk Newborn (SARAR) constitutes a longitudinal follow-up initiative for newborns (NB) discharged from the Neonatal Intensive Care Unit (NICU) up to 12 years of age, developed at a reference university hospital located in the North Zone of the city of Rio de Janeiro. The institution acts as a tertiary center for maternal-child care for pregnant women and high-complexity NB from different municipalities of the Metropolitan Region, including cases related to extreme prematurity, hypoxic-ischemic syndromes, congenital malformations and severe neonatal complications.
Implemented in 2014 and maintained continuously to the present moment, the project has consolidated itself as an institutional strategy for longitudinal follow-up of high-risk NB in the context of the Unified Health System (SUS). Its implementation occurred in response to the need to expand and reorganize the care offered after hospital discharge, based on the best scientific evidence, improving the previously existing outpatient follow-up which had lower longitudinality, focusing predominantly on the first year of life. The consolidation of SARAR enabled the progressive expansion of clinical follow-up and neuropsychomotor development monitoring, allowing prolonged follow-up according to the individual needs of each child.
The organization of SARAR is based on the principles of interdisciplinarity, interprofessionality, dialogic interaction and family and child-centered care (Rodrigues; Dias, 2022). Professionals and students from the areas of pediatrics, nursing, physiotherapy, speech-language pathology, nutrition and psychology participate in the project, with one possible undergraduate scholarship holder annually, acting in an integrated manner during consultations and clinical discussions. This structure favors an expanded care approach, simultaneously considering clinical, nutritional, motor, behavioral, psychic and social aspects related to child development (Méio; Rodrigues, 2023).
Its organizational structure involving professionals and students from various health areas favors the construction of comprehensive care that considers not only the child's clinical aspects, but also their family and social context, since social and affective interactions in early life are fundamental for the child's full development, especially those established with their primary caregivers.
Over a little more than a decade of operation, the project has undergone a continuous process of care and academic expansion, incorporating new theoretical frameworks, standardized developmental assessment instruments and technologies applied to neonatal and pediatric care, in addition to the creation of an Instagram social media profile for the project, mainly fed by the undergraduate scholarship holder and the project coordinator, who is also responsible for the annual submission of the report to the university's responsible department for recertification approval.
This entire movement was accompanied by the progressive technical qualification of its members, including participation in stricto sensu graduate programs, professional training and the development of research projects with internal and external partnerships to the university, linked to the neonatal segment.
As the scope of SARAR goes beyond the care provided, it constitutes a permanent space for academic training and scientific production. The project maintains interaction with academic leagues through scientific meetings, conversation circles, and study and discussion groups; as well as fostering and enabling various research studies, including with areas other than health, within the university itself, and also with other national institutions (and, recently, international), all initiated after approval by the hospital's Research Ethics Committee (CEP). Currently, three studies are underway: "Reduction of neonatal morbidity and mortality due to perinatal asphyxia with therapeutic hypothermia induced by a servocontrolled cooling system" (CAAE 65560417.0.0000.525); "Evaluation of the functional and anatomical ocular characteristics of children who suffered perinatal hypoxic-ischemic events" (CAAE 78278024.4.0000.5259), in partnership with the hospital's ophthalmology service; and "Analysis of craniofacial deformations through a low-cost photogrammetric method, using cell phone images" (CAAE 79708624.3.0000.5259), in partnership with the university's School of Engineering.
The construction of this care model proves particularly relevant in the context of the Metropolitan Region of Rio de Janeiro, marked by intense territorial inequalities, socioeconomic vulnerabilities and difficulties in accessing specialized health services (Bortz et al., 2015; Hone et al., 2023). In this scenario, factors such as limited urban mobility, food insecurity, low family income and fragmentation of the care network can compromise the continuity of outpatient follow-up and delay the early identification of developmental alterations (Rodrigues; Dias, 2022). Thus, the project began to incorporate strategies aimed at strengthening the bond with families and reducing follow-up losses.
The care flow begins during the neonatal hospitalization, when eligible NB are identified by the multiprofessional team based on previously established clinical criteria (figure 1). The early approach to families during the NICU stay represents a strategic stage of the care process, allowing initial guidance on the importance of longitudinal follow-up and favoring the construction of a bond between the team and caregivers before hospital discharge. Currently, 164 children are regularly attending their outpatient follow-up.
After hospital discharge, the first outpatient consultation occurs, preferably, between seven and 14 days. This moment is considered critical for initial clinical evaluation, family guidance and adaptation to home care. From this stage onwards, a longitudinal follow-up schedule is established, whose frequency varies according to corrected age, clinical conditions and specific needs of each child.
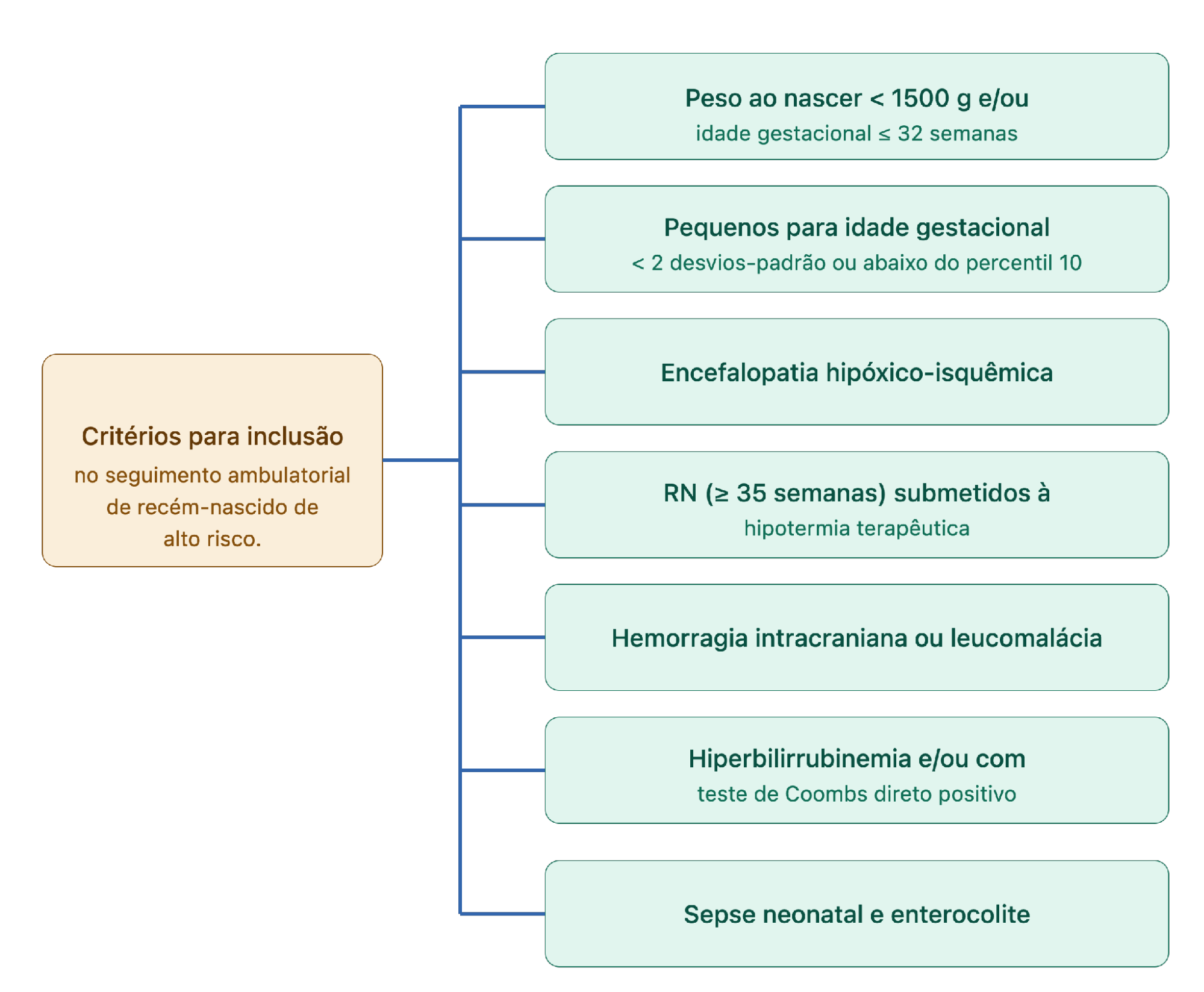
Figure 1: Criteria for inclusion of newborns in the SARAR outpatient clinic. NB: newborn.
Source: Elaborated by the authors.
During the appointments, weight and height growth, neuropsychomotor development, feeding, language, posture and gait, family interaction, behavioral aspects and possible neurological or other organ/system alterations, such as orthopedic ones, are assessed.
Professionals from various undergraduate areas attend to the children and their families simultaneously, in interdisciplinary consultations, in which they apply their knowledge and expertise in a dialogical, collaborative and respectful manner among themselves and appropriate to the culture and understanding of the families. This fosters the production of scientifically based knowledge, returning to the academic community the results of their practices, and being able to offer this assisted population the most reliable conducts, with individuality, comprehensiveness and ecology. The outpatient appointments last about 1 hour, with the participation of faculty and university technical staff from pediatrics, nursing, physiotherapy, speech-language pathology, nutrition and psychology, residents from these various health areas, scholarship undergraduate students and volunteer health students, in three shifts per week.
The appointments are recorded in the hospital's multiprofessional electronic medical record, usually typed by medical professionals; and a multiprofessional form is filled out with clinical and neurodevelopmental data, at key child ages (at the first consultation and at 3, 6, 9, 12, 24 and 36 months and, thereafter, annually), entered into an EPI-INFO 7.0 database (CDC, 2015) by the project's scholarship undergraduate student, with a REDCap database (Harris et al., 2009) currently being developed.
Shared decision-making among professionals favors greater integration of care and reduces the care fragmentation often observed in specialized services. The frequency of follow-up follows the recommendation of the Brazilian Society of Pediatrics (SBP, 2024) (Figure 2).
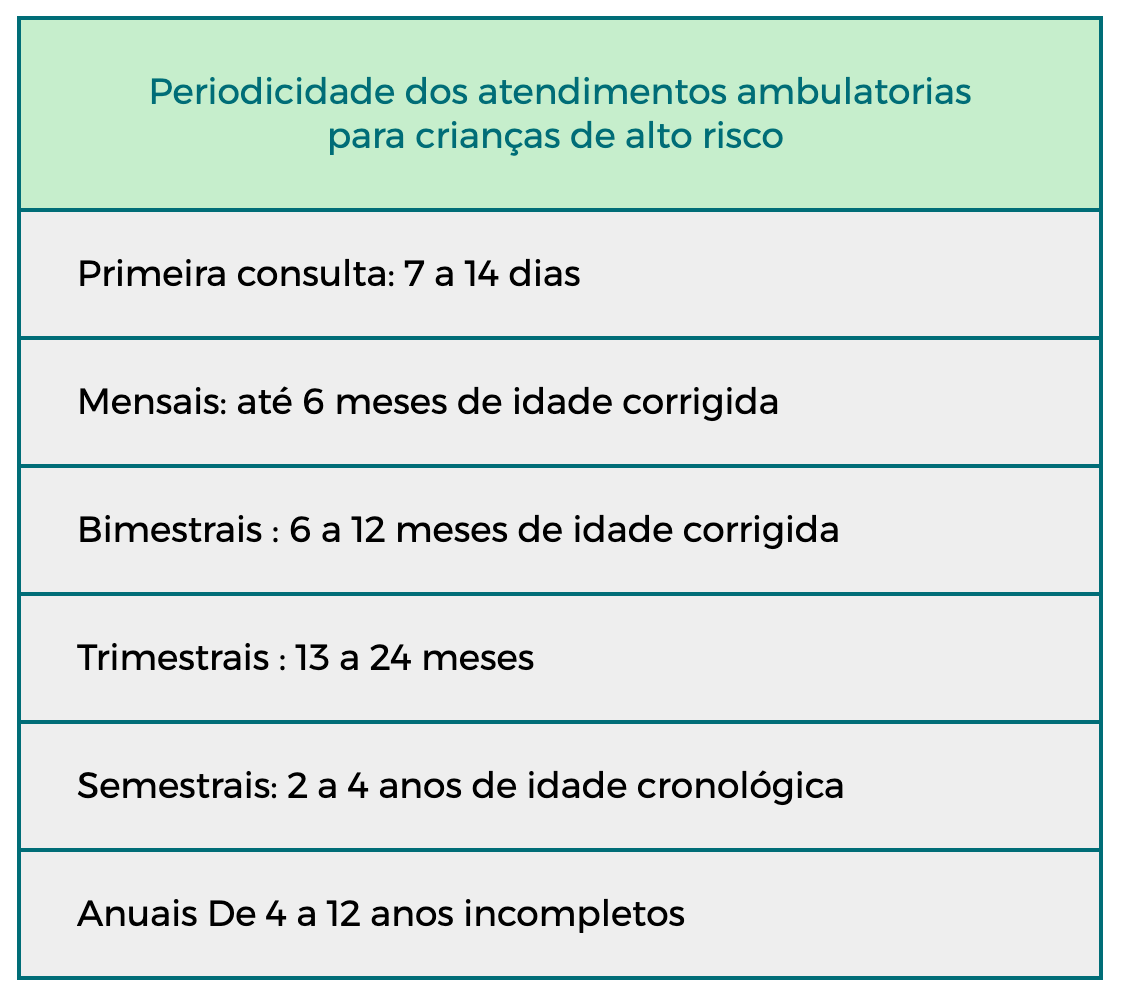
Figure 2: Frequency of outpatient appointments by age group for the follow-up of risk children at SARAR.
Source: SBP; 2024.
The neuropsychomotor development assessment uses validated and internationally recognized instruments, according to the table below, applied according to age group and specific clinical objectives.
Table 1: Screening and diagnostic neurodevelopmental assessment instruments used at SARAR.
Instrument | Age range | Purpose |
Amiel-Tison Examination (clinical neurological examination) | 32 weeks post-conceptual to 6 years | Assesses head circumference, posture, tone (passive/active), reflexes, postural reactions, motor and sensory functions. Clinical tool for early detection of neurological alterations. |
IRDI Protocol - Indicators of Risk for Child Development (screening) | 0 to 18 months | Assesses mother-infant interaction and the child's psychic constitution in the first 18 months of life. Based on 31 clinical indicators divided into four age groups (0–4, 4–8, 8–12 and 12–18 months), observed and/or deduced in the child's development. |
Denver II Screening Test
| 0 to 6 years | Scale with 125 milestones distributed across four areas: gross motor, fine motor-adaptive, language and personal/social. Delay identified when ≥ 2 items are not achieved. |
General Movements Assessment (Prechtl GMA – Qualitative Assessment of General Movements) | Up to 20 weeks post-term | Assesses the quality of spontaneous movements. High sensitivity for risk of cerebral palsy. Applied through video observation. |
Alberta Infant Motor Scale (AIMS) | 40 weeks post-conception to 18 months | Observes movement choices in 4 postures: prone, supine, sitting and standing. Observation measure with minimal handling by the therapist, allowing free movement without assistance or interference from the evaluator. |
HINE – Hammersmith Infant Neurological Examination | 3 to 24 months | Assesses global neurological function by scoring from 0 to 78, based on tone, reflexes, posture and motor response. Especially useful in the early prediction of cerebral palsy (CP), being more accurate when associated with magnetic resonance imaging. |
Bayley III – Diagnostic scale (there are four versions, from 1969 to 2019) | 1 to 42 months | Gold standard in the literature for diagnosing the affected neurodevelopmental domain. Composed of 5 subscales: cognitive, motor, language, social-emotional and adaptive. |
GMFCS – Gross Motor Function Classification System | Up to 18 years | Gross motor function classification system in five levels for children with cerebral palsy: • Level I: Independent walking, without limitations. • Level II: Walking with limitations (long distances/uneven terrain). • Level III: Walking with aid (e.g., walker); wheelchair for long distances. • Level IV: Limited mobility; predominant use of wheelchair. • Level V: Extremely restricted mobility; total dependence for locomotion. |
M-CHAT-R – Modified Checklist for Autism in Toddlers, Revised | 16 to 30 months (emphasis: 18 and 24 months) | Questionnaire applied to parents for screening risk for autism spectrum disorder (ASD). Should be followed by a clinical interview if positive. |
ADL 2 | 1 year to 6 years and 11 months | Composed of two scales: Receptive Language and Expressive Language, allowing separate analysis of each domain and facilitating the identification and degree of language delay. |
Source: Viera; Rodrigues, 2025.
This battery of instruments follows the child's initial psychic constitution and qualifies the developmental assessment, allowing early identification of deviations and timely intervention. The instruments are applied either by the entire team (such as the Denver II test) or by the specialist in the area (for example, the ADL, applied by the team's speech-language pathologist).
Guidance directed to families always permeates this entire process, in the context of parenting, and addresses early stimulation, feeding, immunization, child development and strengthening of the parental bond. Health education constitutes, therefore, a cross-cutting axis of the project, occurring both during appointments and in collective activities held in the waiting room, led by the undergraduate students duly supervised and accompanied by the professionals.
The follow-up of children is performed considering corrected age for premature infants up to two years, regarding growth, nutrition and development. Corrected age for prematurity is the age the child would have if they had been born on their estimated date of delivery (EDD).
Regarding growth, for patients who are up to 50 weeks of post-menstrual age (gestational age at birth + chronological age), data are assessed according to the Fenton curves for weight, height and head circumference for age (Fenton; Elmrayed; Alshaikh, 2025). From 50 weeks onwards, the classification of nutritional status follows the cut-off points recommended by the WHO (WHO, 2006), with the aid of the WHO Anthro program (WHO, 2010) for calculating anthropometric indicators for children under 5 years, and WHO Anthro Plus for those over 5 years (WHO, 2009). The assessment of the patient's food intake, acceptance and tolerance is performed at each consultation through a dietary history and application of a 24-hour dietary recall.
Immunization is performed according to chronological age, with emphasis on passive immunization, with the recent incorporation by the SUS of the monoclonal antibody nirsevimab, for the prevention of respiratory infection by the respiratory syncytial virus, the main cause of hospital readmission in premature infants; and also with emphasis on the use of acellular vaccines, with lower rates of adverse side effects (Rodrigues; Viera, 2025).
Another relevant aspect of the experience refers to the incorporation of technologies applied to the assessment and monitoring of child development. Notably, the use of photogrammetry for the analysis of positional cranial asymmetries, developed in partnership with the cartographic engineering area linked to the university, through a research project (approved by the CEP under number 79708624300005259) aligned with SARAR (Figure 3). This integration evidences the potential of university hospitals as spaces for technological innovation applied to the needs of the SUS.

Figure 3: Assessment of positional cranial asymmetries using three-dimensional photogrammetry carried out in interdisciplinary partnership between the high-risk newborn follow-up outpatient clinic and the university's cartographic engineering area.
Source: Rodrigues et al. (2025)
Beyond the care dimension, the project has an important formative impact. Undergraduate students, residents and graduate students participate actively in clinical activities, case discussions, educational actions and scientific projects, developing competencies related to interprofessional work, comprehensive care and longitudinal attention to high-risk children. For the scholarship undergraduate student, participation, as recommended by the National University Extension Plan, enables experiencing new practices, critically evaluating their training and perceiving the social insertion of their profession, as well as specialized knowledge in a differentiated health situation, with increasing incidence and progressive social impact.
The experience also annually results in the production of scientific papers presented at congresses and academic events, as well as in the publication of articles, all eminently interdisciplinary, contributing to the dissemination of knowledge related to neonatal follow-up and child development.
Despite the advances observed throughout the consolidation of the project, challenges persist related to the continuity of care, especially with regard to follow-up losses associated with social vulnerabilities and the structural difficulties of the urban network. In our latest survey, we observed a follow-up loss of 37%, motivated mainly by illness of the primary caregiver, hospitalization of the child, difficulty in access (lack of financial resources, violence in the community and weather conditions). To address these barriers, strategies such as active search, remote contact with families and the use of digital communication tools have been progressively incorporated into the care routine.
Another challenge encountered by families of high-risk children who evolve with neurodevelopmental alterations is the difficulty in accessing rehabilitation services. The unequal distribution of specialized services, the shortage of qualified professionals, long waiting lists and the need for frequent travel hinder the continuity of multiprofessional follow-up. Furthermore, again, socioeconomic barriers are observed that limit regular attendance at therapies, such as transportation costs, absence of support networks and incompatibility between appointment schedules and family routines. These difficulties can result in delay in the start of early interventions, lower adherence to treatment and discontinuity of clinical follow-up.
As a consequence, these children may present worse motor, cognitive, language and socioemotional development, since early intervention is considered fundamental to enhance brain plasticity in the first years of life. The absence or irregularity in access to therapies can also contribute to the worsening of functional deficits, greater dependence on specialized care throughout life and a negative impact on the quality of life of the child and their family (Dias; Rodrigues; Duarte, 2024). These limitations widen health inequalities, compromising the prognosis and increasing the future demand for more complex services in the public health system.
Despite the challenges faced, we can cite successes over this decade. In this last year, such as the timely identification and interdisciplinary intervention in developmental and growth alterations to minimize sequelae with home guidance and therapeutic referrals, based on the validated instruments used and mentioned above. Thus, of 21 infants evaluated for the detection of possible cranial asymmetries, 15 were identified with cranial asymmetries by measurement using a craniometer performed by the team's physiotherapist and by photogrammetry through the research project in partnership with engineering, coupled to SARAR, with documented improvement verified after physiotherapeutic intervention. Also, Health Education, in the consultation and waiting rooms, interdisciplinary and family-centered, results throughout the project in reports of comfort from primary caregivers, helping them in the affective and technical, multifaceted and challenging dealing with their children. Good news is the creation and implementation of the REDCap database for NB with asphyxia; of the 90 asphyxiated NB discharged from the NICU and referred to SARAR, 66 are in follow-up, with a descriptive analysis of the neonatal profile carried out and developmental results underway. Regarding the prevention and minimization of absenteeism, the control of morbidities and absences with rescheduling allowed us 109 reschedulings in a context of 327 appointments and 124 absences. And, in the psychic/mental sphere, the application of the IRDI in 83 children, between 0 and 18 months, showed signs of psychic distress in 39 and gradual improvement in 25 children, through timely intervention and throughout the follow-up.
It is relevant to state that from the experience of the SARAR extension project, we can verify that the demands of the target population (high-risk children and their respective families) can arise genuinely, which reinforces the potential of extension actions as an instrument of integration between the university, health services and the concrete needs of the population served by the SUS.
4 Conclusion
The experience of the SARAR Project demonstrates that a model of interprofessional, interdisciplinary and dialogical outpatient follow-up of high-risk newborns integrated into the Unified Health System is viable. Over a decade, SARAR has consolidated longitudinal care centered on the child and the family, which favored the timely identification and intervention of alterations in growth and neurodevelopment, health education for caregivers and interdisciplinary training of students and professionals.
On the other hand, the experience also highlighted the challenges related to the continuity of follow-up, bringing to light social vulnerabilities and difficulties in accessing specialized rehabilitation services.
In this sense, it is recommended to strengthen the maternal-child health care network through more effective articulations between maternity wards, primary health care, follow-up outpatient clinics and rehabilitation services. Active search strategies and family support can contribute to the identification and mitigation of these barriers and thus favor the expansion of continuity of care and better outcomes for high-risk children.
References
AMIEL-TISON, C.; GOSSELIN, J. Desarrrollo neurológico de 0 a 6 años: etapas y evaluación. Madrid: Narcea, S.A. de Ediciones, 2006.
AVALIAÇÃO NEUROLÓGICA INFANTIL DE HAMMERSMITH. Tradução e adaptação: Tathiana Ghisi de Souza e Moyra Aloia Romero.
BAYLEY, N. Bayley Scales of Infant and Toddler Development. 3. ed. San Antonio, TX: Pearson, 2006.
BORTZ, M. et al. Disaggregating health inequalities within Rio de Janeiro, Brazil, 2002-2010, by applying an urban health inequality index. Cadernos de Saúde Pública, v. 31, n 1, p. 107-119, nov. 2015. DOI: 10.1590/0102-311x00081214.
BRASIL. Ministério da Saúde. Painel de Monitoramento de Nascidos Vivos. Brasília: Ministério da Saúde, 2025. Available at: https://svs.aids.gov.br/daent/centrais-de-conteudos/paineis-de-monitoramento/natalidade/nascidos-vivos/. Access in: 20 may 2026.
BRASIL. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Atenção à saúde do recém-nascido: guia para os profissionais de saúde. v. 1: Cuidados gerais. 2. ed. atual. Brasília: Ministério da Saúde, 2014.
CENTERS FOR DISEASE CONTROL AND PREVENTION (CDC). Epi Info™. Version 7.2. Atlanta: CDC, 2015. Available at: https://www.cdc.gov/epiinfo/. Access in: 20 may 2026.
DARRAH, J.; PIPER, M.; WATT, M. Assessment of gross motor skills of at-risk infants: predictive validity of the Alberta Infant Motor Scale. Developmental Medicine & Child Neurology, v. 40, n. 7, p. 485-491, 12 nov. 2008. DOI: 10.1111/j.1469-8749.1998.tb15399.x.
DIAS, B. L. S.; RODRIGUES, M. C. C.; DUARTE, J. L. M. B. Quality of life of families and siblings of children with cerebral palsy treated at a reference neurorehabilitation center in Brazil,. Jornal de Pediatria, abr. 2024. Available at: https://doi.org/10.1016/j.jped.2024.03.010. Access in: 10 may 2026.
EINSPIELER, C.; PRECHTL, H. F. Prechtl’s assessment of general movements: a diagnostic tool for the functional assessment of the young nervous system. Mental Retardation and Developmental Disabilities Research Reviews, v. 11, p. 61-67, 2005.
FENTON, T. R.; ELMRAYED, S.; ALSHAIKH, B. N. Fenton third-generation growth charts of preterm infants without abnormal fetal growth: a systematic review and meta-analysis. Paediatric and Perinatal Epidemiology, 19 jun. 2025. Available at: https://doi.org/10.1111/ppe.70035. Access in: 21 maio 2026.
FERREIRA, R.C. et al. Effects of early interventions focused on the family in the development of children born preterm and/or at social risk: a meta-analysis. Jornal de Pediatria, v. 96, n. 1, p. 20-38, jan. 2020. Available at: https://doi.org/10.1016/j.jped.2019.05.002. Access in: 21 may 2026.
FEUERWERKER, L.C.M.; CECÍLIO, L.C.O. O hospital e a formação em saúde: desafios atuais. Ciência & Saúde Coletiva, v. 12, n. 4, p. 965-971, ago. 2007. DOI: 10.1590/s1413-81232007000400018.
HARRIS, P. A. et al. Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, v. 42, n. 2, p. 377-381, 2009. DOI: 10.1016/j.jbi.2008.08.010.
HONE, T. et al. Associations between primary healthcare and infant health outcomes: a cohort analysis of low-income mothers in Rio de Janeiro, Brazil. The Lancet Regional Health - Americas, v. 22, p. 100519, jun. 2023. Available at: https://doi.org/10.1016/j.lana.2023.100519. Access in: 19 may 2026.
HOWSON, C. P. et al. Born Too Soon: preterm birth matters. Reproductive Health, v. 10, S1, nov. 2013. DOI: 10.1186/1742-4755-10-s1-s1.
KUPFER, M. C. M. et al. Predictive value of clinical risk indicators in child development: final results of a study based on psychoanalytic theory. Revista Latinoamericana de Psicopatologia Fundamental, v. 13, n. 1, p. 31-52, mar. 2010. DOI: 10.1590/s1415-47142010000100003.
LOSAPIO, M. F. et al. Checklist Modificado para Autismo em Crianças Pequenas: versão revisada e consulta de seguimento (M-CHAT-R/F). Available at: https://mchatscreen.com/wp-content/uploads/2020/09/M-CHAT-R_F_Brazilian_Portuguese_v2.pdf. Access in: 4 may 2026.
MÉIO, M. D. B. B.; RODRIGUES, M. C. C. Repercussões da prematuridade no crescimento. In: MÉIO, Maria Dalva Barbosa Baker; RODRIGUES, Maura Calixto Cecherelli. Nascimento Prematuro: repercussões no desenvolvimento integral. [S. l.]: Editora FIOCRUZ, 2023. p. 57-74. ISBN 9786557082195. Available at: https://doi.org/10.7476/9786557082195.0005. Access in: 13 may 2026.
MENEZES, M. L. ADL 2 – Avaliação do Desenvolvimento da Linguagem. 2. ed., 2019.
NAÇÕES UNIDAS BRASIL. Agenda 2030 para o Desenvolvimento Sustentável. 2015. Available at: https://brasil.un.org/pt-br/91863-agenda-2030-para-o-desenvolvimento-sustentável. Access in: 18 may 2026.
NOVAK, I. et al. Early, accurate diagnosis and early intervention in cerebral palsy. JAMA Pediatrics, v. 171, n. 9, p. 897, 1 set. 2017. Available at: https://doi.org/10.1001/jamapediatrics.2017.1689. Access in: 15 may 2026.
OLIVEIRA, R. F. et al. Neurological outcomes in neonates treated with therapeutic hypothermia: challenges in a developing country. Arquivos de Neuro-Psiquiatria, v. 82, n. 09, p. 001-008, set. 2024. DOI: 10.1055/s-0044-1790575.
PALISANO, R. et al. Gross Motor Function Classification System: Expanded & Revised. Ontario: Institute for Applied Health Sciences, McMaster University. 2007. Tradução de Daniela Baleroni Rodrigues Silva, Luzia Iara Pfeifer e Carolina Araújo Rodrigues Funayama. Available at: https://canchild.ca/wp-content/uploads/2025/03/GMFCS-ER_Translation-Portuguese2.pdf?license=yes. Access in: 23 may 2026.
PEDUZZI, M. et al. Educação interprofissional: formação de profissionais de saúde para o trabalho em equipe com foco nos usuários. Revista da Escola de Enfermagem da USP, v. 47, n. 4, p. 977-983, ago. 2013. Available at: https://doi.org/10.1590/s0080-623420130000400029. Access in: 11 may 2026.
PIPER, M. C.; DARRAH, J. Avaliação motora do bebê em desenvolvimento: Escala Motora Infantil de Alberta – EMIA. 2. ed. Porto Alegre.
PRECHTL, H. F. R. State of the art: quality of general movements—a critical appraisal. Early Human Development, v. 61, n. 1, p. 1-14, 2001.
RODRIGUES, M. C. C.; DIAS, B. L. S. Desenvolvimento infantil em contextos biológicos adversos, prematuridade e asfixia perinatal: atuação do pediatra. In: Sociedade Brasileira de Pediatria. PROPED C9V1. Porto Alegre: Artmed Panamericana, v. 1, ciclo 9, p. 11-50, 2022.
RODRIGUES, M. C. C. et al. Uso de uma solução fotogramétrica para diagnóstico e acompanhamento de assimetrias cranianas em crianças de alto risco: relato de experiência. In: XVI Congresso de Pediatria do Estado do Rio de Janeiro, 2025, Rio de Janeiro. XVI Congresso de Pediatria do Estado do Rio de Janeiro, 2025.
RODRIGUES, M. C. C.; VIERA, L. L. C. A. Seguimento do prematuro: uma abordagem sumarizada. In: BARBOSA, A. D. M.; VIEIRA, A. A.; BUENO, A. C. (org.). Perinatologia do dia a dia. 1. ed. Rio de Janeiro: Rubio, 2025.
SABATÉS, A. L. Denver II: teste de triagem do desenvolvimento: manual de treinamento. 1. ed. São Paulo: Hogrefe, 2017.
SOCIEDADE BRASILEIRA DE PEDIATRIA. Manual de Seguimento do Recém-nascido de Alto Risco. 2. ed. Departamento Científico de Neonatologia, 2024.
VALENTINI, N. C.; SACCANI, R. Escala Motora Infantil de Alberta: validação para uma população gaúcha. Revista Paulista de Pediatria, v. 29, n. 2, p. 231-238, jun. 2011. DOI: 10.1590/s0103-05822011000200015.
VIERA, L. L. C. A.; RODRIGUES, M. C. C. Seguimento do prematuro. In: Ambulatório de Pediatria [livro eletrônico]. 1. ed. Rio de Janeiro: 2 ML Design, 2025. Série Rotinas Hospitalares. ISBN 978-65-80709-14-4.
VOHR, B.R. et al. Follow-up care of high-risk infants. Pediatrics, Elk Grove Village, v. 123, n. 2, 2009. DOI: 10.1542/peds.114.s5.i.
WORLD HEALTH ORGANIZATION (WHO). Multicentre Growth Reference Study Group: WHO Child Growth Standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: WHO, 2006.
WORLD HEALTH ORGANIZATION (WHO). WHO AnthroPlus for personal computers manual: software for assessing growth of the world's children and adolescents. Geneva: WHO, 2009. Available at: https://www.who.int/tools/growth-reference-data-for-5to19-years/application-tools.
WORLD HEALTH ORGANIZATION (WHO). WHO Anthro for personal computers, version 3.2.2, 2011: software for assessing growth and development of the world's children. Geneva: WHO, 2010.
About the Authors
Maura Calixto Cecherelli de Rodrigues is a pediatrician and neonatologist, associate professor at the Department of Pediatrics of the Faculty of Medical Sciences of the Universidade do Estado do Rio de Janeiro and coordinator of the extension project SARAR (DEPEXT/UERJ); member of the scientific departments of Development and Behavior of the Brazilian Society of Pediatrics and of Development and Rehabilitation of the Society of Pediatrics of the State of Rio de Janeiro.
Alice Valente da Silva is a nutritionist and member of the extension project SARAR (DEPEXT/UERJ), preceptor of the clinical nutrition residency program at Hospital Universitário Pedro Ernesto; master's student in Food and Nutritional Security at the Universidade Federal do Estado do Rio de Janeiro (UNIRIO).
Cirlene de Lima Marinho is a physiotherapist and member of the extension project SARAR (DEPEXT/UERJ); master in Physiology and Clinical and Experimental Physiopathology from the Universidade do Estado do Rio de Janeiro. Preceptor of the Neonatal ICU, Intermediate Nursery and Follow-up Outpatient Clinics for high-risk NB and pediatric patients post-PICU at Hospital Universitário Pedro Ernesto. Faculty of the module on Physiotherapeutic Care for Newborns at Centro Universitário Augusto Motta (UNISUAM).
Daiana Evangelista La Macchia is a speech-language pathologist and member of the extension project SARAR (DEPEXT/UERJ); Specialist in Orofacial Myofunctional Motricity by CFFA, advanced training in Language by CEFAC and Breastfeeding Consultancy course by Instituto Mamebem; master's student in the Professional Master's Program in Telehealth at UERJ.
Edneusa Oliveira Flor is a physiotherapist and member of the extension project SARAR (DEPEXT/UERJ); coordinator of the Motor and Respiratory Pediatric Physiotherapy Outpatient Clinic - Policlínica Piquet Carneiro – UERJ; master in Telehealth from the professional master's program in Telehealth and Telemedicine at UERJ.
Elaine Rego Menezes is a psychologist and member of the extension project SARAR (DEPEXT/UERJ); specialized in Child and Adolescent Psychotherapy by Instituto Fernandes Figueira and coordinator of the Medical Psychology Service of the Perinatal Center at Hospital Universitário Pedro Ernesto.
Eloá Gonçalves de Oliveira Campos is a student in the 10th semester of physiotherapy at UNISUAM, where she is part of the academic league of neurofunctional physiotherapy (LAFIN) and a member of the extension project SARAR.
Gloria Maria Bastos da Silva Bacelar is a pediatrician and neonatologist and member of the extension project SARAR (DEPEXT/UERJ); master in Medical Sciences from UERJ.
João Mario Pereira: is an undergraduate student in the seventh semester of the Faculty of Medical Sciences at UERJ and scholarship holder of the extension project SARAR (DEPEXT/UERJ) for the 2025-2026 biennium.
Lucía Arenas Viera is a pediatrician and neonatologist; doctoral student in the Postgraduate Program in Medical Clinic and with a doctoral thesis linked to the extension project SARAR (DEPEXT/UERJ) (area of neonatal hypoxic-ischemic encephalopathy, with emphasis on therapeutic hypothermia, using a prospective observational design). Master in Medical Sciences from the Universidade do Estado do Rio de Janeiro (UERJ),
Maria Aparecida Thiengo is a nurse and member of the extension project SARAR (DEPEXT/UERJ); master in Women's and Children's Health from FENF/UERJ.
Simone Augusta Ribas is a nutritionist and associate professor at the Universidade Federal do Estado do Rio de Janeiro, post-doctorate in Human Nutrition from UFRJ, and member of the extension project SARAR (DEPEXT/UERJ).
Author Contributions
Conceptualization [MCCR, AVS, CLM]; Methodology [MCCR, AVS, CLM, LAV]; Analysis, drafting, writing and editing, visualization [MCCR, AVS, CLM, DEM, LAV, JMP, EOF, ERM, EGOC, GMBB, MAT, SAR] Supervision [MCCR]; Project administration [MCCR]. All authors have read and agreed to the published version of the manuscript.
Informed Consent
The research encompasses three approvals by ethics committees, and informed consent was obtained from all legal guardians, as well as assent from minor participants over five years of age. The Certificate of Presentation for Ethical Consideration (CAAE) numbers associated with the study are: "Reduction of neonatal morbidity and mortality due to perinatal asphyxia with therapeutic hypothermia induced by a servocontrolled cooling system" (CAAE 65560417.0.0000.525); "Evaluation of the functional and anatomical ocular characteristics of children who suffered perinatal hypoxic-ischemic events" (CAAE 78278024.4.0000.5259), in partnership with the hospital's ophthalmology service; and "Analysis of craniofacial deformations through a low-cost photogrammetric method, using cell phone images" (CAAE 79708624.3.0000.5259), in partnership with the university's School of Engineering.
Conflicts of Interest
The authors declare no conflict of interest.
About Coleção Estudos Cariocas
Coleção Estudos Cariocas (ISSN 1984-7203) is a publication dedicated to studies and research on the Municipality of Rio de Janeiro, affiliated with the Pereira Passos Institute (IPP) of the Rio de Janeiro City Hall.
Its objective is to disseminate technical and scientific production on topics related to the city of Rio de Janeiro, as well as its metropolitan connections and its role in regional, national, and international contexts. The collection is open to all researchers (whether municipal employees or not) and covers a wide range of fields — provided they partially or fully address the spatial scope of the city of Rio de Janeiro.
Articles must also align with the Institute’s objectives, which are:
- to promote and coordinate public intervention in the city’s urban space;
- to provide and integrate the activities of the city’s geographic, cartographic, monographic, and statistical information systems;
- to support the establishment of basic guidelines for the city’s socioeconomic development.
Special emphasis will be given to the articulation of the articles with the city's economic development proposal. Thus, it is expected that the multidisciplinary articles submitted to the journal will address the urban development needs of Rio de Janeiro.