
Volume 14 Issue 2 *Corresponding author flavia.carvalho@ioc.fiocruz.br Submitted 25 May 2026 Accepted 06 Jul 2026 Published 16 Jul 2026 Citation SOUZA, A. L. M. M. F. et al. Spatial distribution and maternal-infant epidemiological profile of live births with orofacial clefts in the state of Rio de Janeiro between 2014 and 2023. Coleção Estudos Cariocas, v. 14, n. 2, 2026.
DOI: 10.71256/19847203.14.2.236.2026 The article was originally submitted in PORTUGUESE. Translations into other languages were reviewed and validated by the authors and the editorial team. Nevertheless, for the most accurate representation of the subject matter, readers are encouraged to consult the article in its original language.


| Spatial distribution and maternal-infant epidemiological profile of live births with orofacial clefts in the state of Rio de Janeiro between 2014 and 2023 Distribuição espacial e perfil epidemiológico materno-infantil dos nascidos vivos com fendas orofaciais no estado do Rio de Janeiro entre 2014 e 2023 Distribución espacial y perfil epidemiológico materno-infantil de los nacidos vivos con fisuras orofaciales en el estado de Río de Janeiro entre 2014 y 2023 Ana Luiza Meneguci Moreira Franco de Souza1, Ana Clara Rodrigues Moreira Gomes2, Luiz Felipe Rodrigues de Souza3, Maria Clara Barbosa Ferreira de Franca4, Rafaela Coimbra Neves Mattos5 e Flávia Martinez de Carvalho6* 1Programa de Pós-Graduação em Genética da Universidade Federal do Rio de Janeiro, Rua Professor Rodolpho Paulo Rocco - Cidade Universitária, Rio de Janeiro/RJ, 21941-617,
ORCID: 0000-0002-5753-0585, analuizameneguci@gmail.com 2Programa de Pós-Graduação Stricto sensu em Biologia Celular e Molecular do Instituto Oswaldo Cruz, Fiocruz, Av. Brasil, 4365 - Manguinhos, Rio de Janeiro/RJ, 21040-360,
ORCID: 0009-0004-1221-1320, anasrmg16@gmail.com 3Programa de Pós-Graduação em Genética da Universidade Federal do Rio de Janeiro, Rua Professor Rodolpho Paulo Rocco - Cidade Universitária, Rio de Janeiro/RJ, 21941-617,
ORCID: 0009-0003-7406-2730, lfrsdesouza@gmail.com 4Instituto Oswaldo Cruz - Fiocruz (Laboratório de Epidemiologia das Malformações Congênitas), Av. Brasil, 4365 Pavilhão Leônidas Deane - Manguinhos, Rio de Janeiro/RJ, 21040-360,
ORCID: 0009-0005-1326-7921, clarabarbosaferre@gmail.com 5Instituto Oswaldo Cruz - Fiocruz (Laboratório de Epidemiologia das Malformações Congênitas), Av. Brasil, 4365 Pavilhão Leônidas Deane - Manguinhos, Rio de Janeiro/RJ, 21040-360,
ORCID: 0009-0001-0346-9424, rafaelacnmattos@gmail.com 6Instituto Oswaldo Cruz - Fiocruz (Laboratório de Epidemiologia das Malformações Congênitas), Av. Brasil, 4365 Pavilhão Leônidas Deane - Manguinhos, Rio de Janeiro/RJ, 21040-360,
ORCID: 0000-0003-2617-9689, flavia.carvalho@ioc.fiocruz.br
AbstractOrofacial clefts (OFCs) are congenital anomalies that impact child development. We conducted the ecological-spatial analysis and the maternal-infant epidemiological profile of live births with OFCs in Rio de Janeiro, by health regions, using SINASC data (2014–2023). The mean prevalence of OFCs ranged from 3.5 to 6.7 per 10,000 live births. Baía da Ilha Grande, Serrana, and Noroeste showed the highest prevalences, below national and global estimates, suggesting underreporting. There was a higher frequency among preterm infants, males, and those with low Apgar scores. 23.3% of the cases were associated with other anomalies, mainly musculoskeletal. Keywords: orofacial clefts, epidemiology, SINASC, health regionalization, maternal and child profile, spatial analysis ResumoAs fendas orofaciais (FO) são anomalias congênitas que impactam o desenvolvimento infantil. Realizamos a análise ecológica-espacial e traçamos o perfil epidemiológico materno-infantil dos nascidos vivos (NV) com FO no Rio de Janeiro, por regiões de saúde, com dados do SINASC (2014–2023). A prevalência média de FO variou de 3,5 a 6,7 por 10.000 NV. Baía da Ilha Grande, Serrana e Noroeste apresentaram maiores prevalências, abaixo das estimativas nacionais e globais, sugerindo subnotificação. Houve maior frequência em prematuros, no sexo masculino e com baixos escores de Apgar. 23,3% dos casos estavam associados a outras anomalias, principalmente musculoesqueléticas. Palavras-chave: fendas orofaciais, epidemiologia, SINASC, regionalização em saúde, perfil materno-infantil, análise espacial
ResumenLas fisuras orofaciales (FO) son anomalías congénitas que afectan el desarrollo infantil. Realizamos un análisis ecológico-espacial y el perfil epidemiológico materno-infantil de los nacidos vivos (NV) con FO en Río de Janeiro, por regiones de salud, utilizando datos del SINASC (2014–2023). La prevalencia media de FO osciló entre 3,5 y 6,7 por 10.000 NV. Baía da Ilha Grande, Serrana y Noroeste presentaron las mayores prevalencias, por debajo de las estimaciones nacionales y mundiales, lo que sugiere subregistro. Hubo mayor frecuencia en prematuros, en el sexo masculino y con bajos puntajes de Apgar. 23,3% de los casos estuvieron asociadas con otras anomalías, principalmente musculoesqueléticas. Palabras clave: fisuras orofaciales, epidemiología, SINASC, regionalización en salud, perfil materno-infantil, análisis espacial |
1 Introduction
Orofacial clefts (OFC) constitute one of the most prevalent groups of congenital anomalies (CA) worldwide. They result from failures in the embryonic facial processes that form the upper lip and/or palate between the fourth and twelfth weeks of gestation (Mossey, P. et al., 2009). OFCs present wide phenotypic variability and are classified according to the affected anatomical structure, the main types being cleft lip (CL), cleft palate (CP), and cleft lip and palate (CLP) (Leslie; Marazita, 2013). About 30% of cases are part of a syndromic condition, such as Van der Woude Syndrome (Spritz, 2001). However, isolated cases are the majority and have a complex etiology, with both genetic and environmental components (Cobourne, 2004). Among the environmental factors involved, the consumption of alcohol (DeRoo et al., 2008) (relative risk (RR) of 2.2); smoking (Little; Cardy; Munger, 2004) (RR = 1.34 for CL and CLP); and teratogenic drugs (e.g., topiramate with a 6.26 increased risk for CP) (Alsaad; Kaplan; Koren, 2015) during pregnancy stand out.
The prevalence of OFC varies according to ethnic groups, geographic areas, sex, and socioeconomic status (Mossey, P. A. et al., 2011). OFCs entail several repercussions for the individual's health and the family unit, as they compromise important aspects of growth and development from birth, such as feeding difficulties, speech development, greater predisposition to hearing disorders, and psychosocial implications, such as low self-esteem and risk of social isolation (Freitas et al., 2012). Regarding mortality, a Brazilian study with data from 1996 to 2023 identified 987 deaths associated with OFC in Brazil, with respiratory and cardiovascular disorders being the main associated causes (Costa et al., 2025). These data reinforce the importance of a multidisciplinary team for continuous follow-up regarding both the physical aspect and family support (Franco; Gonçalves; Franco, 2000).
The Information System on Live Births (SINASC) is a population database with information on births in Brazil (Pedraza, 2012). The base document for recording information in SINASC is the Live Birth Declaration (DNV), mandatory throughout the national territory, and essential for the systematic recording of births and surveillance of CAs. Currently, the DNV has 52 variables distributed across 8 blocks. Two fields are responsible for information on CAs: field 6, where the presence or absence of CA is indicated, and field 41, where all diagnosed CAs are described and coded (Brazil. Ministry of Health, 2022). The coding of OFCs in SINASC is divided into three main groups: Q35 – CP, Q36 – CL, Q37 – CLP, and is carried out following the Ministry of Health's guidelines based on the International Statistical Classification of Diseases and Related Health Problems – ICD-10. The records may present detailing of up to three digits, with the third digit used to specify characteristics such as laterality and extent of the involvement (World Health Organization, 2016).
Through the analysis of SINASC data, it is possible to assess the distribution of OFCs in the territory, identifying areas with higher concentration (Predebon et al., 2010). Thus contributing to the formulation of hypotheses about risk factors and the identification of differences in access to health services, supporting the planning and organization of maternal and child care (Oliveira et al., 2015), given that recently Law No. 15,133/2025, sanctioned on May 6, 2025, established the mandatory provision of reconstructive surgery by the Unified Health System (SUS).
There is a gap in epidemiological studies on OFC published in the state of Rio de Janeiro; therefore, this approach proves to be fundamental due to the territorial and healthcare inequalities built throughout history, the concentration of medium and high-complexity services in the capital, and the weaknesses in the regional articulation of the SUS, which results in the impairment of comprehensive care and equitable access to health services (Rodrigues; Souza; Cabral, 2025). Considering the hypothesis that regional prevalences below the national average could reflect differential underreporting, the present study aims to analyze the spatial distribution and the maternal-child epidemiological profile of live births (LB) with OFC in the state of Rio de Janeiro, according to health regions, using SINASC data from 2014 to 2023.
2 Materiais e métodos
2.1 Tipo de estudo
This is a descriptive and retrospective epidemiological study, with a cross-sectional approach and spatial analysis. We highlight that although the study presents a time series, it is not a longitudinal approach, as there was no follow-up of cases over time. The health regions of the state of Rio de Janeiro were used as units of analysis, allowing the observation of the spatial and temporal distribution of OFC prevalences over ten years.
2.2 Study area and period
The study was conducted based on records of LB from 2014 to 2023, in the health regions of the state of Rio de Janeiro, located in the Southeast region of Brazil. The health regions were defined according to an agreement established at the 10th Ordinary Meeting of the Bipartite Interagency Commission of the State of Rio de Janeiro (CIB/RJ), established by CIB Deliberation No. 1452, of November 9, 2011. The state consists of nine health regions: Baía da Ilha Grande, Baixada Litorânea, Centro-Sul, Médio Paraíba, Metropolitana I, Metropolitana II, Noroeste, Norte, and Serrana (Bipartite Interagency Commission, 2011). For analytical purposes, in this study, the Metropolitana I and Metropolitana II regions were grouped into the "Metropolitana" category, according to the standardization of the database used.
2.3 Data source and study population
Data were obtained through the Health Applied Data Science Platform (PCDaS), developed by the Oswaldo Cruz Foundation (Fiocruz, ICICT, 2026), based on SINASC (Brazil. Ministry of Health, 2024). The study population consisted of all LB of mothers residing in the state of Rio de Janeiro, from 2014 to 2023, with records of OFCs identified by ICD-10 codes: ICD-Q35 (cleft palate), ICD-Q36 (cleft lip), and ICD-Q37 (cleft lip and palate) (World Health Organization, 2016).
2.4 Data analysis
Records with valid information on the congenital anomaly code and the health region code of residence were included. Data organization, processing, and analysis were performed in the Google Colaboratory environment (Google Colab), using the Python programming language. The mean prevalence of OFCs per health region was calculated from the ratio between the number of cases and the total number of LB in the same location and period, multiplied by 10,000. Since the aim of the study was to analyze OFC cases in general, without detailing the types of clefts, records that presented more than one code for OFC were counted only once.
For spatial analysis purposes, restricted to descriptive cartographic visualization, the health region code of residence was used to allocate records to health regions, which were subsequently cross-referenced with the official cartographic base of the health regions of the state of Rio de Janeiro, made available by the Government of the State of Rio de Janeiro and modified by the Data Science Nucleus (NCD) (Public Prosecutor's Office of the State of Rio de Janeiro, 2020). Subsequently, the mean prevalences over the studied period (2014 to 2023) were calculated for each health region. These means were used to construct a thematic map in QGIS software (QGIS Development Team, 2024), representing the spatial distribution of the mean prevalence of OFCs among the health regions of the state of Rio de Janeiro. The time series of prevalences was constructed from the annual calculation of OFC prevalences, allowing the assessment of the evolution of the event over the period from 2014 to 2023.
2.4.1 Maternal and child variables
Regarding the other variables of the study, the following database fields were considered: maternal age, maternal education, maternal race/color, gestational age, month of initiation of prenatal care, one-minute Apgar score, five-minute Apgar score, and sex. Fields filled with "ignored" were disregarded in the variables in which they were present (supplementary material). Prevalence according to maternal-child variables was calculated for these eight variables, considering the number of cases and the total number of LB in each category. From these estimates, means of the prevalences over the studied period were calculated. The option for calculating mean prevalences was adopted as an exploratory strategy to identify possible variations between the years of the studied period, and subsequently, a summary mean of these estimates was obtained, with the aim of facilitating the visualization of the patterns observed over the period and reducing random variations.
Maternal age was categorized into five age groups: up to 20 years, 21–25 years, 26–30 years, 31–35 years, and over 35 years. Gestational age was divided into three categories that can be correlated with the division performed by the World Health Organization (Blencowe et al., 2013): up to 27 weeks (corresponding to extreme preterm), between 28 and 36 weeks (corresponding to very preterm and moderate preterm), and 37 weeks or more (corresponding to term and post-term births). We categorized maternal education into elementary school I, elementary school II, high school, incomplete higher education, and complete higher education. Maternal race/color was divided into White, Brown (Parda), and Black (Preta). Month of initiation of prenatal care divided into trimesters. Sex: male and female. One-minute and five-minute Apgar scores were categorized as less than 7 or between 7–10, since Apgar values above 7 are considered indicators of good fetal vitality (COFN; ACOG, 2015). Additionally, the categories "no schooling" (maternal education) and "Yellow" and "Indigenous" (maternal race/color) were excluded from the analysis due to the small number of observations (corresponding to 0.1% and 0.4% of total births, respectively), which could compromise the stability and robustness of the prevalence estimates. In cases with more than one code for congenital anomalies (in addition to cleft codes), the most recurrent anomalies were analyzed, grouped by anatomical systems, following the blocks of chapter XVII of the ICD-10 (World Health Organization, 2019).
2.5 Ethical aspects
As this is a study with secondary, public, anonymized data, with no possibility of individual identification of participants, the present research does not require review by a Research Ethics Committee, as established by Resolution No. 510, of April 7, 2016, of the National Health Council (Brazil. Ministry of Health, 2016).
3 Results and discussion
3.1 Prevalence of orofacial clefts in Rio de Janeiro
In the period from 2014 to 2023, 1,030 cases of OFC were recorded in the state of Rio de Janeiro (total values by health region presented in the supplementary material), the mean prevalence of OFC ranged between 3.5 and 6.7 cases per 10,000 LB, with the highest rates concentrated in the health regions of Baía da Ilha Grande, Serrana, and Noroeste (Figure 1). According to the epidemiological bulletin on CAs from the Ministry of Health, between 2010 and 2022, OFCs corresponded to the third most prevalent group of CAs in the country, with a prevalence of 7 cases per 10,000 LB (Saúde, 2023). The study by Vieira et al. (2025), which analyzed OFC cases in Brazil between 2010 and 2021, found a mean prevalence for OFC in Brazil of 6.7 cases per 10,000 LB. However, worldwide, the prevalence of OFC is 14.7 per 10,000 LB (Panamonta et al., 2015).
In view of the national and global panorama, the prevalence observed in the various health regions of Rio de Janeiro is below expectations, especially the Norte, Centro-Sul, and Baixada Litorânea regions. One possible justification for this difference is the fact that there is still significant underreporting of CAs in Brazil (Saúde, 2023), which often stems from a lack of awareness among health professionals regarding the recording and correct coding of CAs.
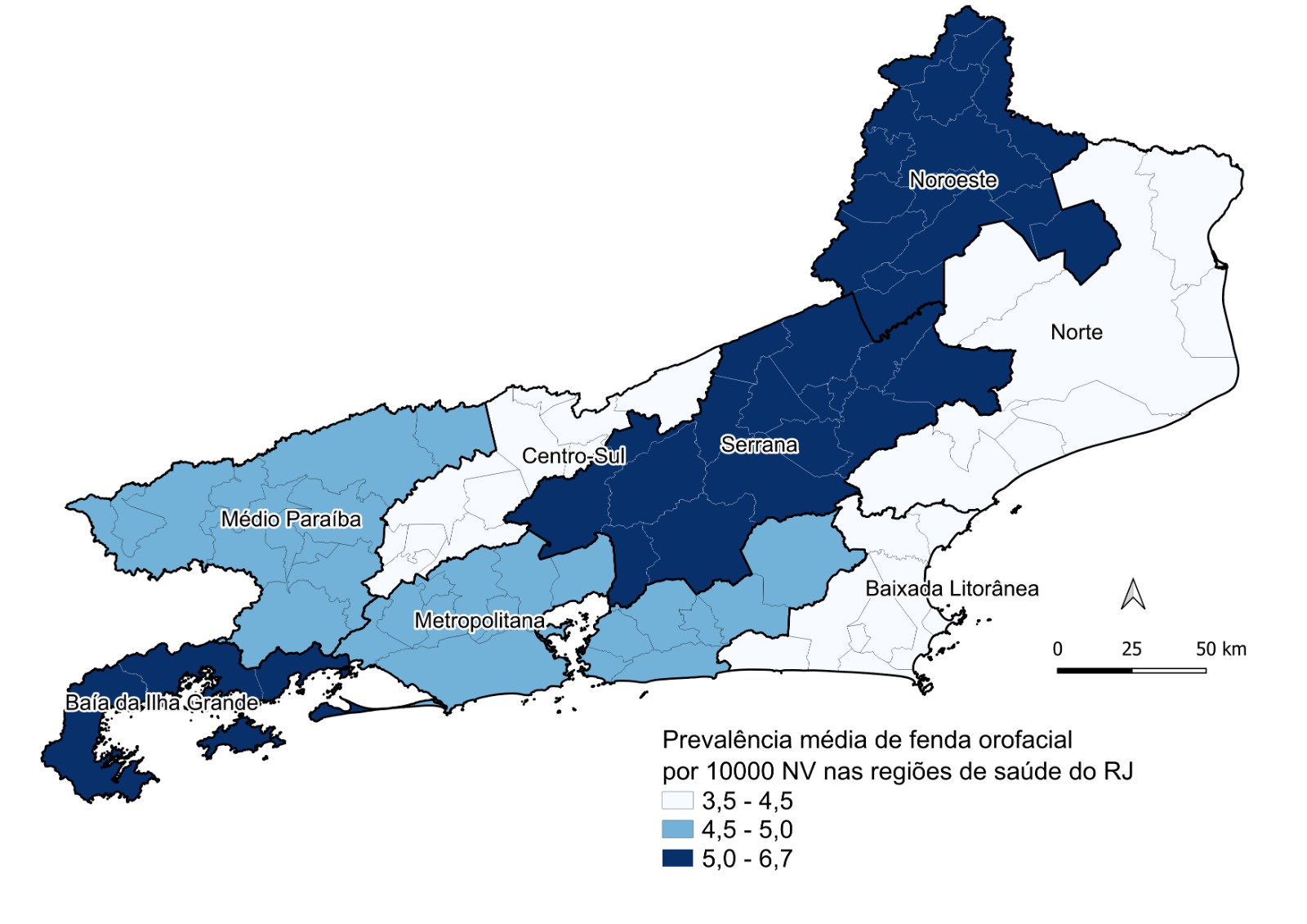
Figure 1: Spatial distribution of the mean prevalence of orofacial cleft per 10.000 LB in the health regions of the state of Rio de Janeiro, from 2014 to 2023.
Source: The authors
Corroborating this scenario, a study conducted in the city of Rio de Janeiro identified low agreement between CA diagnoses recorded in hospital medical records (performed or confirmed after birth and during hospitalization) and those reported in Live Birth Declarations. For OFCs, agreement values were only 36.8% and 23.7% for records with two and three digit coding in categories Q35, Q36, and Q37, respectively, evidencing important inconsistencies in the completion of these documents (Guerra et al., 2008).
The temporal analysis of prevalences revealed heterogeneous behavior among health regions (Figure 2), highlighting the stability of the Metropolitana region (bringing together the Metropolitana I and II health regions) at around 5 cases per 10,000 LB (Figure 2E), as well as the marked fluctuation in Baía da Ilha Grande, which recorded peaks of up to 15 cases in 2022 (Figure 2A). The oscillations in Baía da Ilha Grande may be related to the smaller number of births in the region, making rates more susceptible to annual variations.
In contrast, the more constant pattern in the Metropolitana region may reflect the high population concentration, which brings together about 75% of the state's population, and consequently, a larger number of births, reducing sharp variations in rates. Furthermore, the greater availability of health services in the Metropolitana region may favor the diagnosis and notification of cases (Kuschnir et al., 2010). It is also noteworthy that even the prevalence peaks detected in the studied period did not significantly exceed the worldwide prevalence.
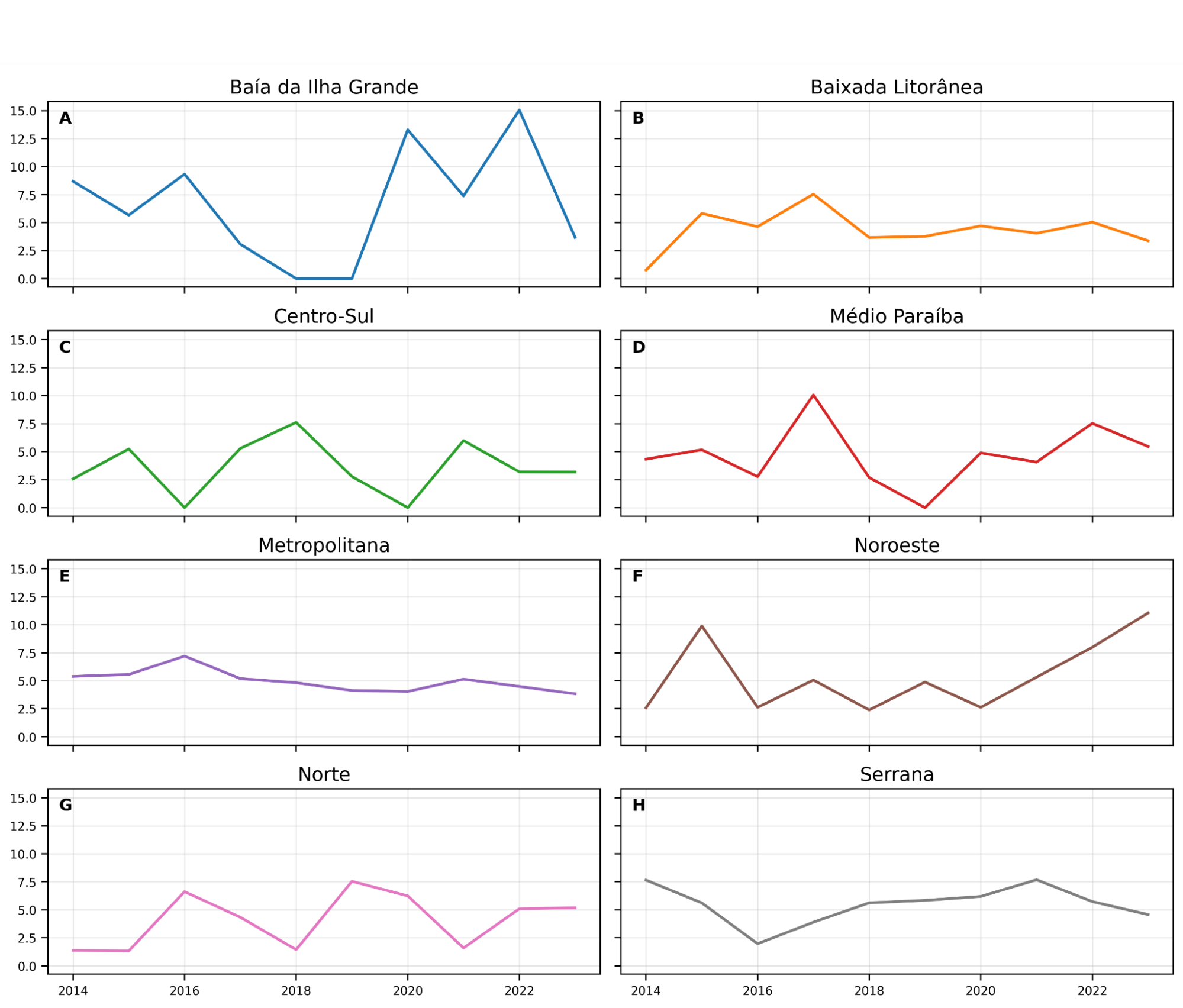
Figure 2: Temporal trend of annual prevalences of orofacial cleft per 10,000 LB in the health regions of the state of Rio de Janeiro, from 2014 to 2023.
Source: The authors
3.2 Maternal-child epidemiological profile
The analysis of maternal characteristics allowed a better understanding of the epidemiological profile found in OFC cases in Rio de Janeiro (total values detailed by health region and by year can be found in the supplementary material). The schooling variable did not present a consistent pattern among regions that would suggest a clear relationship with OFC prevalence (Figure 3A). However, as this is a descriptive analysis, such variations should be interpreted with caution, considering the possible instability of estimates in regions with a smaller number of births and OFC cases. The Metropolitana region stood out for exhibiting similar prevalences among schooling categories. The PCDaS database already aggregates the Metropolitana I and II regions, which supports the use of the single 'Metropolitana' category in the analysis. Even so, it is recognized that this aggregation may mask important internal heterogeneities between these areas.
Previous studies have investigated the relationship between maternal and/or paternal schooling and the occurrence of OFC in Brazil, although the results remain heterogeneous. Figueiredo et al. (2015), in a retrospective case-control study conducted in the state of Mato Grosso with 80 mothers of children with and without OFC, observed a higher prevalence of OFC among mothers with lower educational and socioeconomic levels. Altoé, Borges, Neves et al. (2020), in a case-control study conducted in the same state with 150 mothers of children with CLP and 300 mothers of children without CAs, identified low paternal schooling as a risk factor for OFC. The paternal schooling variable was not tested in our sample since these data are not available in SINASC.
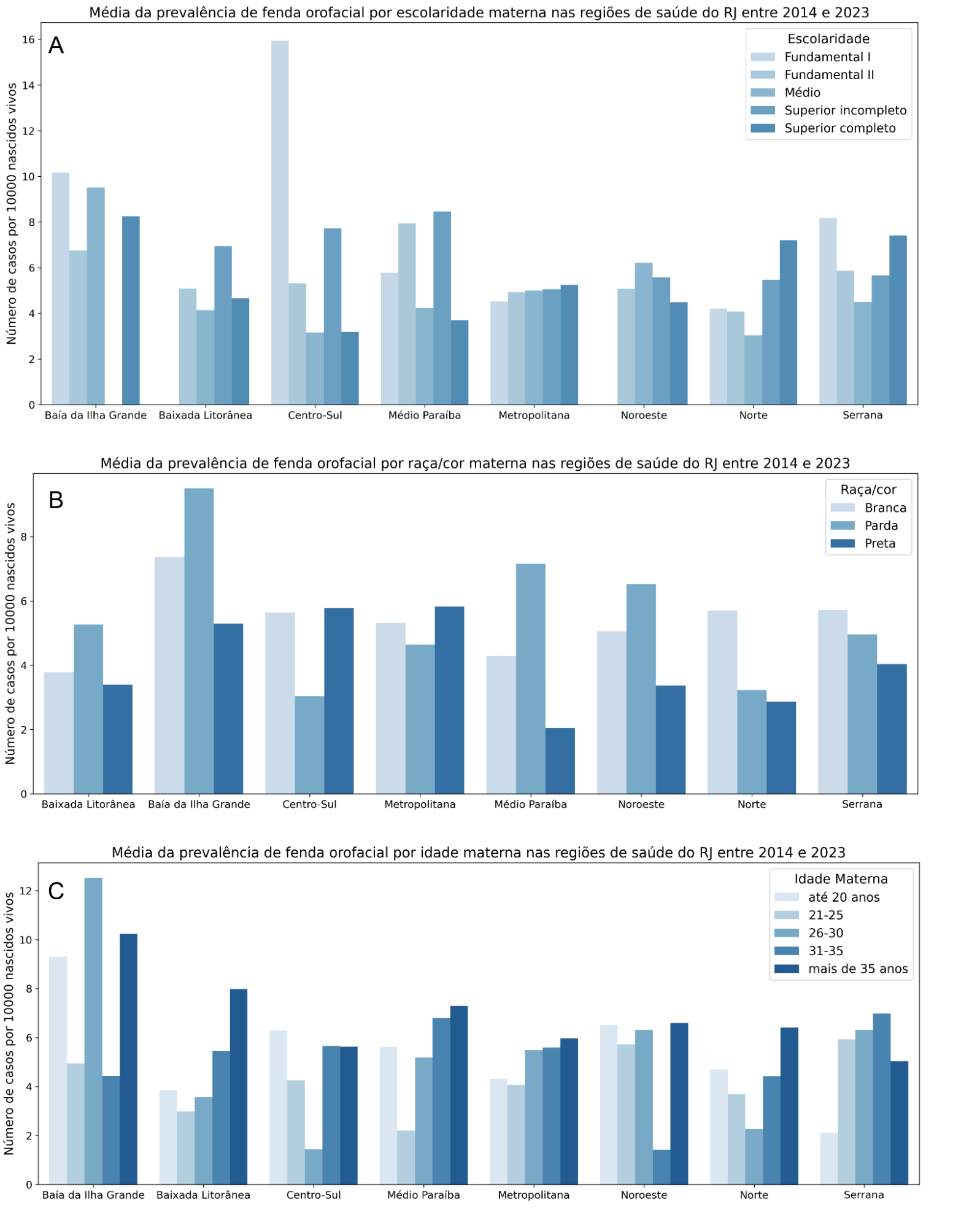
Figure 3: Distribution by health region of Rio de Janeiro of the prevalence of orofacial clefts by maternal epidemiological characteristics. A: Schooling; B: Race/Color; C: Age.
Source: The authors
On the other hand, Campos Neves et al. (2016), Silva, Calumby and Freitas (2024), and Santos et al. (2025) present convergent results in not identifying a consistent pattern between parental schooling and the occurrence of OFC. Campos Neves et al. (2016), in a cross-sectional study conducted in Mato Grosso with 116 patients, evaluated the schooling of both parents and observed no influence of this factor on the occurrence of OFC. Silva, Calumby and Freitas (2024), in a descriptive study based on SINASC data (1999–2020) on isolated OFCs in Brazil, analyzed maternal schooling and did not identify a consistent pattern of association with the occurrence of OFC. Santos et al. (2025), in an ecological study also of national scope with SINASC data (2001–2022), did not observe higher frequencies among mothers with lower schooling and higher OFC rates.
The analysis of maternal schooling as a determinant of maternal-child health is also supported in an international context. Baron et al. (2015) demonstrated in a cross-sectional study conducted with 6,711 pregnant women attended in primary care in the Netherlands that women with lower schooling were more likely to smoke, to be exposed to passive smoking, to have low belief in health control, not to attend childbirth preparation classes, and not to take folic acid supplementation during pregnancy, which may lead to adverse gestational outcomes, such as CAs.
The mean prevalence of OFC showed variations among the health regions of the state of Rio de Janeiro according to maternal race/color in the period from 2014 to 2023 (Figure 3B). In general, higher prevalences were observed among children of Brown (Parda) mothers in half of the health regions analyzed, with emphasis on Baía da Ilha Grande, which presented the highest value among all groups evaluated. In the Médio Paraíba, Baixada Litorânea, and Noroeste regions, higher prevalences were also recorded among Brown mothers. In contrast, some regions presented higher prevalences among White mothers, such as the Norte and Serrana regions. Among Black (Preta) mothers, the values were more heterogeneous, with relatively high prevalences in the Centro-Sul and Metropolitana regions, while the lowest value was observed in Médio Paraíba.
Despite regional variations, there is no consistent pattern between maternal race/color and higher prevalence of OFC. As this is a descriptive analysis, these variations should be interpreted with caution, considering the possible instability of estimates in some regions. It is important to note that the race/color variable has good data completeness in SINASC (Coelho et al., 2023); however, it is a self-declared variable that reflects historical, cultural, and political dimensions of ethnic-racial self-belonging. In this sense, Chor et al. (2019) compared genomic ancestry data, racial composition of census tracts, and individual socioeconomic factors with self-declared race/color in a cohort of 15,105 Brazilians, demonstrating that ancestry alone does not explain self-declared race/color. Complementarily, the study by Nunes et al. (2025) had as one of its objectives to understand the effects of intense miscegenation on Brazilian genetic diversity, describing the population as tri-hybrid, resulting from the predominant contribution of European, African, and Amerindian ancestors. For the state of Rio de Janeiro, contributions of approximately 52% European, 40% African, and 8% Amerindian were estimated.
Maternal age showed a pattern of increasing prevalence towards both age extremes (under 20 years and over 35), with some exceptions, such as in the Baía da Ilha Grande and Serrana regions (Figure 3C). Bille et al. (2005), when analyzing about 1.5 million live births in Denmark, showed an association between higher maternal and paternal age and increased risk for OFC. Similarly, the findings of the meta-analysis by Herkrath et al. (2012) with studies from Europe, the Americas (South, Central, and North), Asia, and Oceania indicated that advanced maternal age presents a distinct association according to the type of OFC. No significant relationship was observed between mothers aged 35 or older and the occurrence of CL or CLP, although when observing only mothers aged 40, there was a 1.56-fold increased risk of having children with CL or CLP compared to those between 20 and 29 years. For CP, a significant increase in odds was found already among mothers aged 35 to 39 years, remaining elevated in mothers aged 40 or older, who had a 1.28-fold higher risk compared to the reference group. The same meta-analysis did not identify a statistically significant association between maternal age <20 years and the occurrence of OFC. In Brazil, with data from Rio Grande do Sul, Maurique et al. 2023 also observed an association between advanced maternal age and CLP or CL.
Lower levels of schooling and family income have been associated with lower use of prenatal care, which can negatively impact the promotion of maternal-child health (Carvalho; Araújo, 2007). The study by Fernandes et al. (2025) reported that mothers who did not have access to prenatal care had an increased risk of having a child with CAs when compared to those who started follow-up in the first trimester. Lopes, Guida and Andrade (2022) observed that the occurrence of CAs is inversely proportional to the number of prenatal consultations. Corroborating the literature, our data show an increase in OFC prevalence when follow-up begins in the second or third trimester. More markedly, the prevalence was higher in the Baía da Ilha Grande and Centro-Sul health regions when considering the third trimester (Figure 4A), although causality cannot be established from a descriptive cross-sectional study.
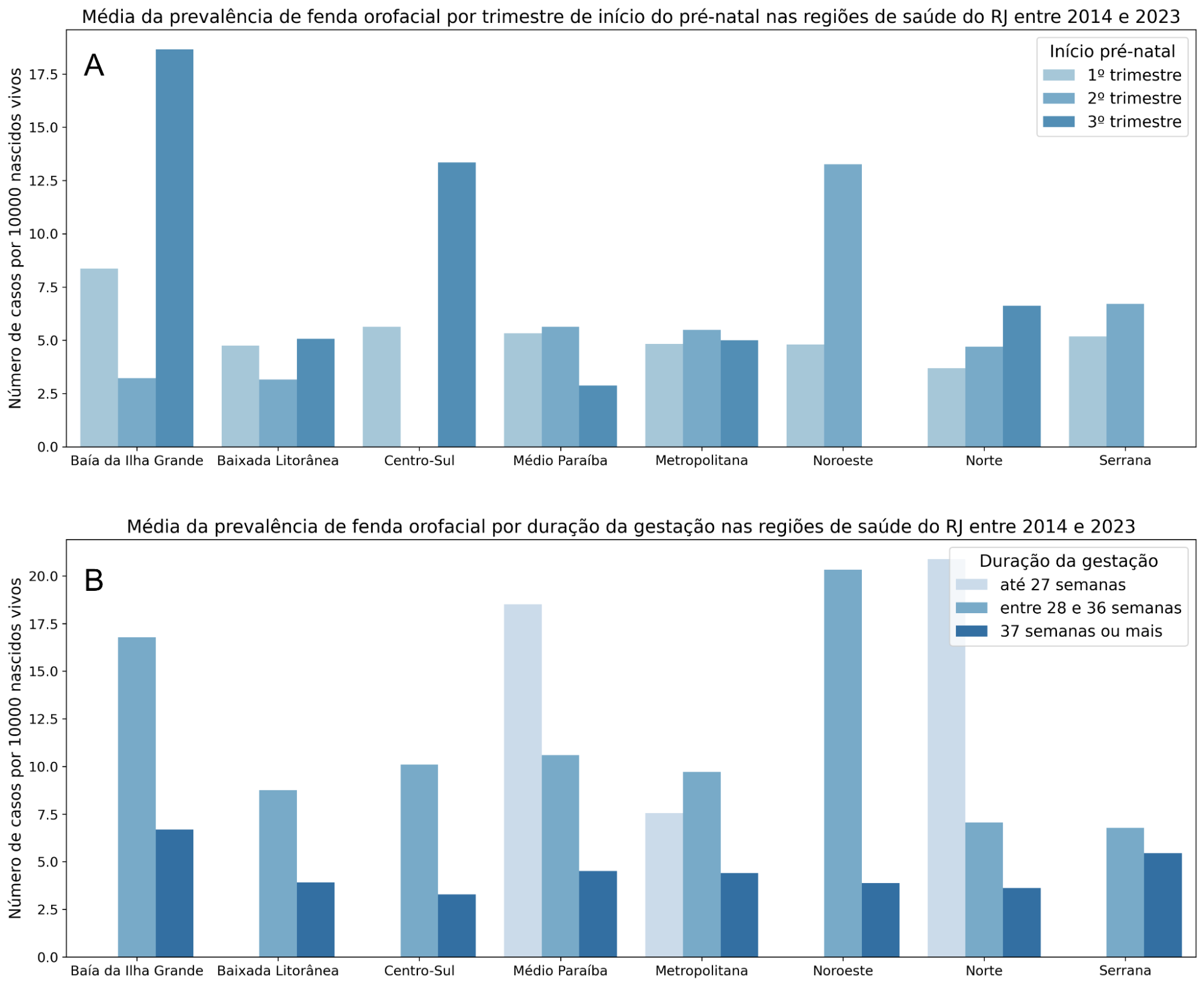
Figure 4: Distribution by health region of Rio de Janeiro of the prevalence of orofacial clefts by gestational epidemiological characteristics. A: Initiation of prenatal care; B: Gestational age.
Source: The authors
These results indicate late follow-up, since much of embryonic development occurs during the first three months, which compromises the window of opportunity for periconceptional supplementation. A population-based case-control study demonstrated that periconceptional supplementation with folic acid was associated with an approximately 60% reduction in the risk of OFC (Xu et al., 2021). In this context, late initiation or non-performance of prenatal care compromises not only gestational monitoring but also the opportunity for guidance and provision of periconceptional supplementation, whose period of greatest effectiveness corresponds precisely to the weeks preceding and following conception. Currently, daily supplementation of 400 to 800 µg of folic acid is recommended for women planning to become pregnant, in addition to the mandatory fortification of flours and other staple foods. This preventive strategy, widely consolidated for neural tube defects, has already been adopted by about 60 countries and contributes to the prevention of approximately one quarter of preventable cases of these CAs worldwide (Kancherla, 2023).
Regarding gestational weeks, it is possible to observe a significant increase in OFC prevalence in births before 36 weeks (Figure 4B), indicating an increased frequency of prematurity among individuals affected by OFC. Clusters with increased prevalence of OFCs in Brazil have also been related to increased preterm birth rates (Santos et al., 2025); this phenomenon can be observed in all health regions of Rio de Janeiro. In the analysis by Silva, Freitas and Vieira (2025), comparing OFC cases from the United States and Brazil between 2017 and 2021, it was found that infants born with OFC in Brazil had a significantly higher chance of preterm birth and that their mothers had fewer than 10 prenatal consultations.
The sex variable showed a higher prevalence in males in all health regions analyzed (Figure 5A). In the literature, a higher prevalence of CL with or without CP (CL/P) is described in males, while CP presents a higher prevalence in females. However, CL/P is the most common type of OFC, representing about 75% of cases (Mossey; Modell, 2012), which may reflect in the prevalences found in the regions of Rio de Janeiro, considering all types of OFC together. Silva, Macari et al. (2022), when analyzing SINASC data from all over Brazil between 2008 and 2017, identified an association between OFC cases, male sex, and preterm birth. From our results, it is possible to infer that the state of Rio de Janeiro also follows this national trend.
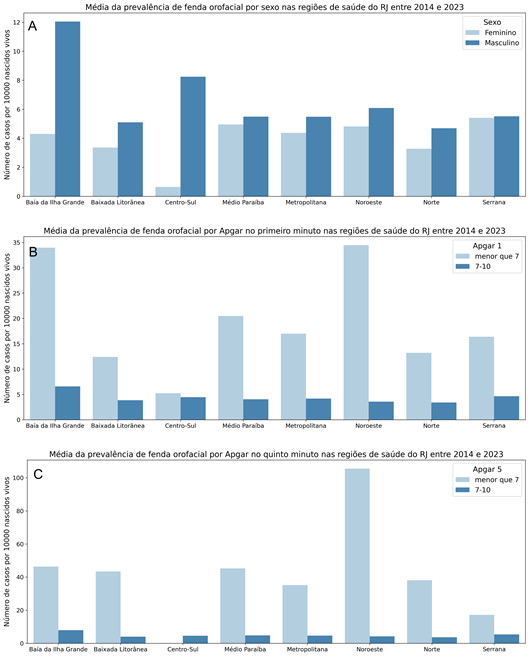
Figure 5: Distribution by health region of Rio de Janeiro of the prevalence of orofacial clefts by newborn epidemiological characteristics. A: Sex; B: One-minute Apgar; C: Five-minute Apgar.
Source: The authors
In all health regions, higher prevalences of OFC were observed in births with an Apgar score below 7 at the first (Figure 5B) and fifth minute of life (Figure 5C), mostly with prevalences above the national average of 7 cases per 10,000 births. Wyszynski and Wu (2002), in a case-control study in the United States, observed that infants born with OFC had a higher frequency of Apgar scores lower than 7 at the fifth minute when compared to controls. The Apgar score is a method of rapid clinical assessment of the newborn and an important screening method; its measurement is performed at the 1st and 5th minute of life to verify adaptation to extrauterine life and identify newborns who need immediate assistance. Apgar values above 7 indicate good neonatal vitality, while Apgar values of 0-3 at the fifth minute are related to an eight-fold increased risk of neonatal death (Casey; McIntire; Leveno, 2001). The higher prevalences of prematurity and low Apgar scores observed reinforce the clinical fragility of these newborns, requiring specialized care to ensure better survival conditions and neonatal prognosis.
The analysis of cases with multiple congenital anomalies allowed the identification of the anatomical systems most frequently associated with OFCs in the state of Rio de Janeiro between 2014 and 2023 (Figure 6). In total, 240 cases were identified that simultaneously presented ICD-10 codes for OFC and for other congenital anomalies, corresponding to 23.3% of all cases recorded in the studied period. Among these records, cases with up to five distinct congenital anomaly codes were observed.
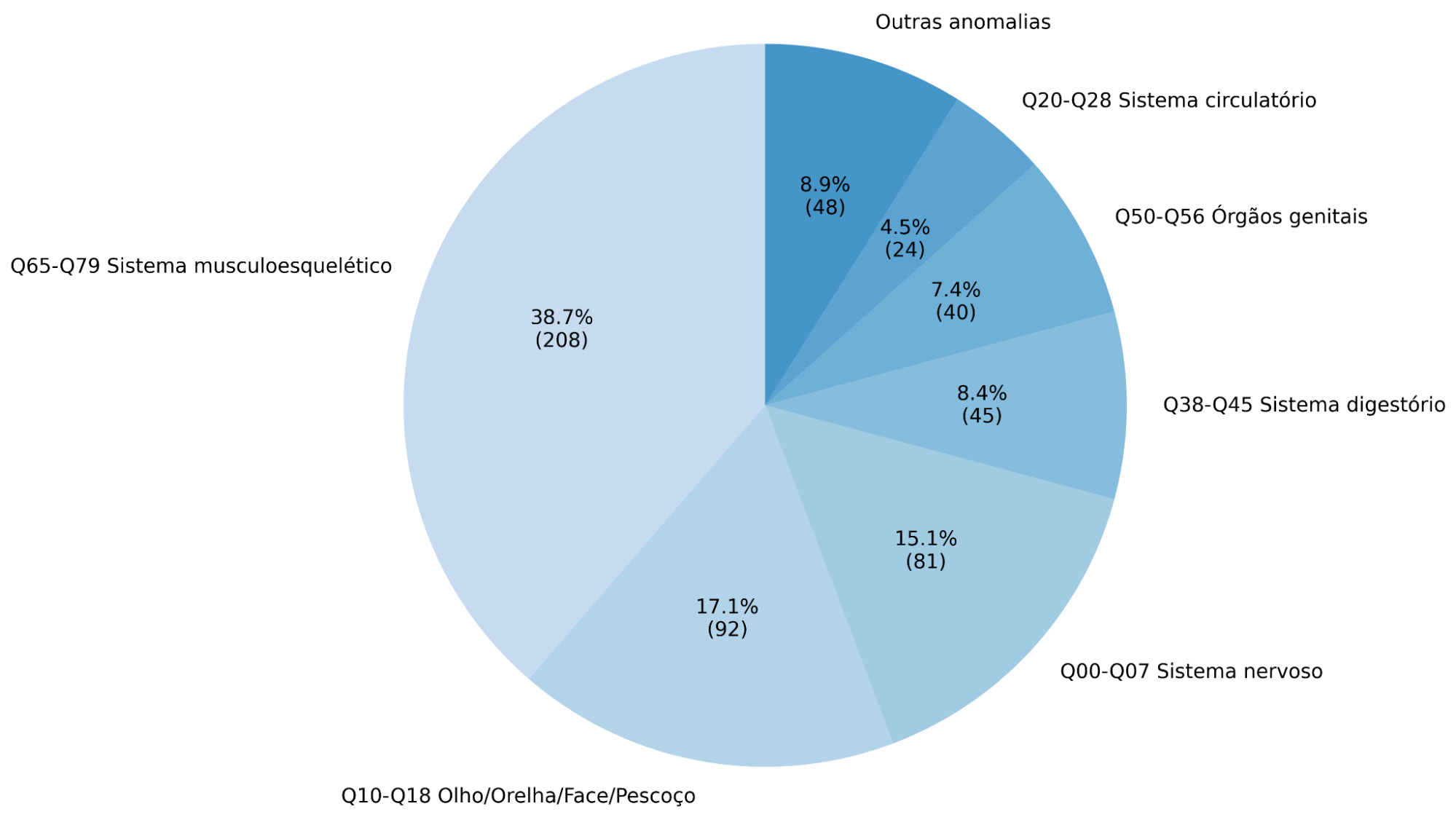
Figure 6: Main groups of congenital anomalies associated with cases of orofacial clefts in the state of Rio de Janeiro between 2014 and 2023.
Source: The authors
The musculoskeletal system was the group with the highest number of records, with 208 in total; among the anomalies of this system, unspecified polydactyly (Q699) stood out with 24 records, followed by other congenital deformities of the foot (Q668). The second most prominent group was congenital anomalies of the eye, ear, face, and neck with 92 records; among these, anomaly of ear position (Q174) and other specified congenital anomalies of the ear (Q178) totaled 30. In third place was the group of anomalies of the nervous system, with a total of 81, highlighting unspecified congenital hydrocephalus (Q038) with 19 records and microcephaly (Q02) with 15 records.
In the study by Stoll, Alembik, and Roth (2022), which analyzed more than 300,000 births in Europe, anomalies of the eyes, face, ear, and neck were identified as the most frequently associated with OFC, followed by musculoskeletal anomalies, diverging from what was found in Rio de Janeiro. Positive associations with OFCs have already been observed with other congenital anomalies, such as anencephaly, encephalocele, congenital clubfoot, and ear anomalies, which are part of the most frequent anatomical groups in the state (Rittler et al., 2008).
As a limitation, the study did not perform statistical tests of association between maternal-child variables, health regions, and the occurrence of OFC, being restricted to descriptive and graphical analysis, which prevents the estimation of association measures and limits inference beyond the description of the observed patterns.
Finally, the findings of this study reinforce that OFCs represent an important public health problem in the state of Rio de Janeiro, not only due to their frequency, but also due to the correlation with clinical conditions that can increase neonatal vulnerability. The identification of higher prevalences in preterm newborns and those with low Apgar scores, in addition to numerous cases with multiple congenital anomalies, evidences the complexity of care for these individuals and the need for a multidisciplinary approach.
The prevalences found are below global and national averages; therefore, the possibility of underreporting in SINASC must be considered. In this context, the strengthening of epidemiological surveillance actions and the training of professionals for the identification and adequate coding of OFCs become fundamental for the planning of public policies and the care network, especially after the enactment of Law 15.133/2025. In general, underestimated prevalences can compromise the adequate distribution of resources, impacting the supply of specialized beds, multidisciplinary teams, and funding allocated to the care of these patients.
4 Conclusion
The analysis of the spatial distribution and epidemiological profile, based on SINASC data, revealed a birth prevalence of OFCs in Rio de Janeiro between 3.5 and 6.7 cases per 10,000 LB, values lower than the global and national averages, which may suggest underreporting. The mapping by health regions evidenced a higher concentration of cases in the Baía da Ilha Grande, Serrana, and Noroeste regions. A more pronounced temporal fluctuation was observed in Baía da Ilha Grande, possibly associated with the smaller number of births, while the Metropolitana region presented greater stability. Among the cases analyzed, a pattern of higher prevalence of OFCs was verified with late initiation of prenatal care in maternal variables. Regarding infant variables, higher prevalences of OFC were observed with prematurity, in males, and low Apgar scores. These findings characterize the maternal-child epidemiological profile of OFCs in the state and highlight the relevance of SINASC as a tool for epidemiological surveillance and support for health planning, by evidencing regional patterns and inequalities that can support the formulation of more targeted public policies.
It is suggested that future studies use linkage strategies between databases (such as SINASC, the Mortality Information System, and the Primary Care Health Information System) to improve record validation and reduce possible underreporting. Furthermore, analytical studies with more robust designs are recommended, capable of investigating risk factors associated with OFCs and explaining the observed regional variations. The findings of this study reinforce the importance of continuous monitoring of OFCs and their articulation with public health policies, in line with Law No. 15,133/2025, contributing to the planning and organization of the reconstructive surgery care network in the state of Rio de Janeiro.
References
ALSAAD, Abdulrahman M.; KAPLAN, Yusuf C.; KOREN, Gideon. First trimester exposure to topiramate and the risk of oral clefts in the offspring: A systematic review and meta-analysis. Reproductive Toxicology, v. 53, p. 45–50, 2015. DOI: 10.1016/j.reprotox.2015.03.003.
ALTOÉ, Regina S.; BORGES, Átila H.; NEVES, A. T. S. C. et al. Influence of Parental Exposure to Risk Factors in the Occurrence of Oral Clefts. Journal of Dentistry (Shiraz), v. 21, n. 2, p. 119–126, 2020. DOI: 10.30476/DENTJODS.2019.77620.0. Available at: https://doi.org/10.30476/DENTJODS.2019.77620.0. Access in: 22 may 2026.
BARON, Romy et al. Socio-demographic inequalities across a range of health status indicators and health behaviours among pregnant women in prenatal primary care: a cross-sectional study. BMC Pregnancy and Childbirth, v. 15, p. 261, 2015. DOI: 10.1186/s12884-015-0676-z. Available at: https://doi.org/10.1186/s12884-015-0676-z. Access in: 21 may 2026.
BILLE, Camilla et al. Parent’s Age and the Risk of Oral Clefts. Epidemiology, v. 16, n. 3, p. 311–316, 2005. DOI: 10.1097/01.ede.0000158745.84019.c2. Available at: https://pubmed.ncbi.nlm.nih.gov/15824545/. Access in: 7 may 2026.
BLENCOWE, Hannah et al. Born Too Soon: The Global Epidemiology of 15 Million Preterm Births. Reproductive Health, BioMed Central, v. 10, Suppl 1, s2, 2013. DOI: 10.1186/1742-4755-10-S1-S2.
BRASIL. MINISTÉRIO DA SAÚDE. Declaração de Nascido Vivo: manual de instruções para preenchimento. 4. ed. Brasília: Ministério da Saúde, 2022. Available at: https://bvsms.saude.gov.br/bvs/publicacoes/declaracao_nascido_ vivo_manual_4ed.pdf. Acceso in: 8 may 2026.
BRASIL. MINISTÉRIO DA SAÚDE. Sistema de Informações sobre Nascidos Vivos (SINASC). Brasília, DF: [s.n.], 2024. Base de dados do DATASUS. Available at: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/. Access in: 4 may 2026.
BRASIL. MINISTÉRIO DA SAÚDE, Conselho Nacional de Saúde. Resolução nº 510, de 7 de abril de 2016. Dispõe sobre as normas aplicáveis a pesquisas em Ciências Humanas e Sociais. Brasília, DF: [s.n.], 24 mai. 2016. Available at: https://conselho.saude.gov.br/resolucoes/2016/Reso510.pdf. Access in: 29 abr. 2026.
CAMPOS NEVES, A. T. et al. Environmental Factors Related to the Occurrence of Oral Clefts in a Brazilian Subpopulation. Nigerian Medical Journal, v. 57, n. 3, p. 167–172, 2016. DOI: 10.4103/0300-1652.184064. Available at: https://doi.org/10.4103/0300-1652.184064. Access in: 22 may 2026.
CARVALHO, Valéria Cristina Pereira de; ARAÚJO, Tereza Virgínia Bezerra de. Adequação da assistência pré-natal em gestantes atendidas em dois hospitais de referência para gravidez de alto risco do Sistema Único de Saúde, na cidade de Recife, Estado de Pernambuco. Revista Brasileira de Saúde Materno Infantil, v. 7, n. 3, p. 309–317, 2007. DOI: 10.1590/S1519-38292007000300010. Available at: https://doi.org/10.1590/S1519-38292007000300010. Access in: 10 may 2026.
CASEY, Brian M.; MCINTIRE, Donald D.; LEVENO, Kenneth J. The Continuing Value of the Apgar Score for the Assessment of Newborn Infants. New England Journal of Medicine, v. 344, n. 7, p. 467–471, 2001. DOI: 10.1056/NEJM200102153440701. Available at: https://www.nejm.org/doi/full/10.1056/NEJM200102153440701. Access in: 7 may 2026.
CHOR, Dora et al. Context-Dependence of Race Self-Classification: Results from a Highly Mixed and Unequal Middle-Income Country. PLoS ONE, v. 14, n. 5, e0216653, 2019. DOI: 10.1371/journal.pone.0216653. Available at: https://doi.org/10.1371/journal.pone.0216653. Access in: 10 may 2026.
COBOURNE, Martyn T. The Complex Genetics of Cleft Lip and Palate. European Journal of Orthodontics, v. 26, n. 1, p. 7–16, 2004. DOI: 10.1093/ejo/26.1.7. Available at: https://academic.oup.com/ejo/article-abstract/26/1/7/568137. Access in: 7 may 2026.
COELHO, R. et al. Nota técnica: O quesito raça/cor no DataSUS: evolução e determinantes da completude. Instituto de Estudos para Políticas de Saúde, São Paulo, v. 30, n. 30, p. 1–9, 2023.
COFN; ACOG. The Apgar Score, American Academy of Pediatrics Committee on Fetus and Newborn and American College of Obstetricians and Gynecologists Committee on Obstetric Practice. Pediatrics, v. 136, n. 4, p. 819–822, 2015. DOI: 10.1542/peds.2015-2651.
COMISSÃO INTERGESTORES BIPARTITE. Deliberação CIB nº 1452, de 09 de novembro de 2011: Aprova a configuração das regiões de saúde do estado do Rio de Janeiro. Rio de Janeiro: CIB/RJ, 2011. Available at: http://www.cib.rj.gov.br/deliberacoes-cib-80-2011/novembro/1221deliberacoes-cib-no-1452-de-09-de-novembro-de-2011.html. Access in: 4 may 2026.
COSTA, Amanda de Andrade et al. Mortality Associated with Orofacial Clefts in Brazil. Dentistry Journal, v. 13, n. 7, p. 282, 2025. DOI: 10.3390/dj13070282. Available at: https://www.mdpi.com/2304-6767/13/7/282. Access in: 7 may 2026.
DEROO, Lisa A. et al. First-Trimester Maternal Alcohol Consumption and the Risk of Infant Oral Clefts in Norway: A Population-based Case-Control Study. American Journal of Epidemiology, v. 168, n. 6, p. 638–646, 2008. DOI: 10.1093/aje/kwn186.
FERNANDES, Qeren Hapuk Rodrigues Ferreira et al. Maternal and Gestational Factors Associated with Congenital Anomalies Among Live Births: A Nationwide Population-Based Study in Brazil from 2012 to 2020. BMC Pregnancy and Childbirth, v. 25, p. 678, 2025. DOI: 10.1186/s12884-025-07675-0. Available at: https://link.springer.com/article/10.1186/s12884-025-07675-0. Access in: 10 may 2026.
FIGUEIREDO, R. F. et al. O papel do ácido fólico na prevenção da fissura orofacial: um estudo epidemiológico. Oral Diseases, v. 21, n. 2, p. 240–247, 2015. DOI: 10.1111/odi.12256. Available at: https://doi.org/10.1111/odi.12256. Access in: 21 may 2026.
FIOCRUZ, ICICT. Plataforma de Ciência de Dados aplicada à Saúde (PCDaS). Rio de Janeiro: [s.n.], 2026. Plataforma de dados em saúde. Available at: https://pcdas.icict.fiocruz.br/. Access in: 29 abr. 2026.
FRANCO, Diogo; GONÇALVES, Luiz Fernando; FRANCO, Talita. Perfil do Tratamento de Fissurados no Brasil. Revista Brasileira de Cirurgia Plástica, v. 15, n. 3, p. 21–32, 2000. Available at: https://www.rbcp.org.br/details/249/Perfil-doTratamento-de-Fissurados-no-Brasil?idioma=pt-BR. Access in: 7 may 2026.
FREITAS, José Alberto de et al. Rehabilitative Treatment of Cleft Lip and Palate: Experience of the Hospital for Rehabilitation of Craniofacial Anomalies/USP (HRAC/USP) – Part 1: Overall Aspects. Journal of Applied Oral Science, v. 20, n. 1, p. 9–15, 2012. DOI: 10.1590/S1678-77572012000100003. Available at: https://doi.org/10.1590/S1678-77572012000100003. Access in: 8 may 2026.
GUERRA, Fernando Antônio Ramos et al. Confiabilidade das informações das declarações de nascido vivo com registro de defeitos congênitos no Município do Rio de Janeiro, Brasil, 2004. Cadernos de Saúde Pública, v. 24, n. 2, p. 438–446, 2008. DOI: 10.1590/S0102-311X2008000200023. Available at: https://doi.org/10.1590/S0102-311X2008000200023. Access in: 7 may 2026.
HERKRATH, Ana Paula Queiroz et al. Parental age as a risk factor for non-syndromic oral clefts: A meta-analysis. Journal of Dentistry, v. 40, n. 1, p. 3–14, 2012. DOI: 10.1016/j.jdent.2011.10.002. Available at: https://www.sciencedirect.com/science/article/abs/pii/S0300571211002417. Access in: 21 may 2026.
KANCHERLA, Vijay. Neural Tube Defects: A Review of Global Prevalence, Causes, and Primary Prevention. Child’s Nervous System, v. 39, n. 7, p. 1703–1710, 2023. DOI: 10.1007/s00381-023-05910-7. Available at: https://doi.org/10.1007/s00381-023-05910-7. Access in: 10 may 2026.
KUSCHNIR, Rosana et al. Regionalização no estado do Rio de Janeiro: o desafio de aumentar acesso e diminuir desigualdades. In: POLÍTICAS e Sistema de Saúde no Brasil. [S.l.]: Editora Fiocruz, 2010. DOI: 10.7476/9788575415924.0011. Available at: https://doi.org/10.7476/9788575415924.0011. Access in: 10 may 2026.
LESLIE, Elizabeth J.; MARAZITA, Mary L. Genetics of Cleft Lip and Cleft Palate. American Journal of Medical Genetics Part C: Seminars in Medical Genetics, v. 163C, n. 4, p. 246–258, 2013. DOI: 10.1002/ajmg.c.31381. Available at: https://pubmed.ncbi.nlm.nih.gov/24124047/. Access in: 7 may 2026.
LITTLE, Julian; CARDY, Allan; MUNGER, Ronald G. Tobacco smoking and oral clefts: a meta-analysis. Bulletin of the World Health Organization, v. 82, n. 3, p. 213–218, 2004.
LOPES, Ester Rocha; GUIDA, Giovana Rocha; ANDRADE, Lucas Alves de. Retrato das anomalias congênitas no estado do Tocantins. Facit Business and Technology Journal, v. 1, n. 35, p. 51–60, 2022. Available at: https://revistas.faculdadefacit.edu.br/index.php/JNT/article/view/1501. Access in: 7 may 2026.
MAURIQUE, L. S. et al. Higher maternal age is associated with higher occurrence of cleft lip/palate in neonates under intensive care. Brazilian Journal of Oral Sciences, v. 2, 2023. DOI: 10.20396/bjos.v22i00.8669246
MINISTÉRIO PÚBLICO DO ESTADO DO RIO DE JANEIRO. Portal Geo MPRJ. Rio de Janeiro: [s.n.], 2020. Available at: https://geo.mprj.mp.br/. Access in: 10 may 2026.
MOSSEY, Peter et al. Cleft Lip and Palate. The Lancet, v. 374, n. 9703, p. 1773–1785, 2009. DOI: 10.1016/S0140-6736(09)60695-4. Available at: https://doi.org/10.1016/S0140-6736(09)60695-4. Access in: 8 may 2026.
MOSSEY, Peter A.; MODELL, Bernadette. Epidemiology of Oral Clefts 2012: An International Perspective. Frontiers of Oral Biology, v. 16, p. 1–18, 2012. DOI: 10.1159/000337464. Available at: https://doi.org/10.1159/000337464. Access in: 7 may 2026.
MOSSEY, Peter A. et al. Global Oral Health Inequalities: Challenges in the Prevention and Management of Orofacial Clefts and Potential Solutions. Advances in Dental Research, v. 23, n. 2, p. 247–258, 2011. DOI: 10.1177/0022034511402083. Available at: https://pubmed.ncbi.nlm.nih.gov/21490237/. Access in: 7 may 2026.
NUNES, Kelly et al. Admixture’s Impact on Brazilian Population Evolution and Health. Science, v. 388, n. 6746, eadl3564, 2025. DOI: 10.1126/science.adl3564. Available at: https://doi.org/10.1126/science.adl3564. Access in: 21 may 2026.
OLIVEIRA, Max Moura et al. Avaliação do Sistema de Informações sobre Nascidos Vivos. Brasil, 2006 a 2010. Epidemiologia e Serviços de Saúde, v. 24, n. 4, p. 629–640, 2015. DOI: 10.5123/S1679-49742015000400005. Available at: https://www.scielo.br/j/ress/a/bRpxYCk4zyh4NwK84yyTKFj/abstract/?lang=pt. Access in: 7 may 2026.
PANAMONTA, Vipawee et al. Global Birth Prevalence of Orofacial Clefts: A Systematic Review. Journal of the Medical Association of Thailand, v. 98, Suppl. 7, s11–s21, 2015. Available at: https://pubmed.ncbi.nlm.nih.gov/26742364/. Access in: 7 may 2026.
PEDRAZA, D. F. Qualidade do Sistema de Informações sobre Nascidos Vivos (SINASC). Ciência e Saúde Coletiva, v. 17, n. 10, p. 2729–2737, 2012. DOI: 10.1590/S1413-81232012001000021.
PREDEBON, Kelen Marja et al. Desigualdade sócio-espacial expressa por indicadores do Sistema de Informações sobre Nascidos Vivos (SINASC). Cadernos de Saúde Pública, v. 26, n. 8, p. 1583–1594, 2010. DOI: 10.1590/S0102-311X2010000800012. Available at: https://www.scielo.br/j/csp/a/Kx88vDDRWVgTQbZvdHjn8Pw/?lang=pt. Access in: 7 may 2026.
QGIS DEVELOPMENT TEAM. QGIS Geographic Information System. [S.l.]: Open Source Geospatial Foundation Project, 2024. Software livre de sistema de informação geográfica. Available at: https://qgis.org/. Access in: 29 apr. 2026.
RITTLER, Monica et al. Preferential Associations between Oral Clefts and Other Major Congenital Anomalies. The Cleft Palate-Craniofacial Journal, v. 45, n. 5, p. 525–532, 2008. DOI: 10.1597/06-250.1. Available at: https://pubmed.ncbi.nlm.nih.gov/18788868/. Access in: 20 may 2026.
RODRIGUES, J. Nunes; SOUZA, A. T. Orozco Morais de; CABRAL, R. da Silva. Política, Território e Desigualdade: os Caminhos da Regionalização da Saúde no Rio de Janeiro: Paths of SUS Regionalization in the Fluminense Context. Revista Espaço e Geografia, v. 28, p. 1–31, 2025. DOI: 10.26512/2236-56562025e58035. Available at: https://doi.org/10.26512/2236-56562025e58035. Access in: 8 may 2026.
SANTOS, Luis Gustavo Souza et al. Nationwide Spatial Patterns and Maternal and Birth-Related Factors Associated with Orofacial Clefts in Brazil. International Journal of Environmental Research and Public Health, v. 22, n. 7, p. 995, 2025. DOI: 10.3390/ijerph22070995. Available at: https://doi.org/10.3390/ijerph22070995. Access in: 10 may 2026.
SAÚDE, Brasil. Ministério da. Análise da situação epidemiológica das anomalias congênitas no Brasil, 2010 a 2022. Brasília, DF: [s.n.], 3 mar. 2023. Available at: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/ boletins/epidemiologicos/edicoes/2024/boletim-epidemiologicovolume-55-no-06. Access in: 1 may 2026.
SILVA, Adriana M. da; FREITAS, V. S.; VIEIRA, Alexandre R. Comparative Study of Individuals Born with Orofacial Clefts in the United States and Brazil. Journal of Neonatal-Perinatal Medicine, v. 18, n. 6, p. 526–532, 2025. DOI: 10.1177/19345798251343829. Available at: https://pubmed.ncbi.nlm.nih.gov/40372708/. Access in: 7 may 2026.
SILVA, Adriana Mendonça da; CALUMBY, Rodrigo Tripodi; FREITAS, Valéria Souza. Epidemiologic profile and prevalence of live births with orofacial cleft in Brazil: a descriptive study. Revista Paulista de Pediatria, v. 42, e2022234, 2024. DOI:10.1590/1984-0462/2024/42/2022234.
SILVA, Raquel S.; MACARI, Soraia et al. The Panorama of Cleft Lip and Palate Live Birth in Brazil: Follow-up of a 10-Year Period and Inequalities in the Health System. The Cleft Palate-Craniofacial Journal, v. 59, n. 12, p. 1490–1501, 2022. DOI: 10.1177/10556656211050004. Available at: https://pubmed.ncbi.nlm.nih.gov/34787490/. Access in: 7 may 2026.
SPRITZ, Richard A. The Genetics and Epigenetics of Orofacial Clefts. Current Opinion in Pediatrics, v. 13, n. 6, p. 556–560, 2001. DOI: 10.1097/00008480-200112000-00011. Available at: https://pubmed.ncbi.nlm.nih.gov/11753106/. Access in: 7 may 2026.
STOLL, Claude; ALEMBIK, Yves; ROTH, Marie-Pierre. Co-occurring anomalies in congenital oral clefts. American Journal of Medical Genetics Part A, 188A, p. 1700–1715, 2022. DOI: 10.1002/ajmg.a.62689. Available at: https://doi.org/10.1002/ajmg.a.62689. Access in: 20 may 2026.
VIEIRA, Karoline Machado et al. Orofacial clefts in newborns in Brazil: a time series study, 2010–2021. Epidemiologia e Serviços de Saúde, v. 34, 2025. DOI: 10.1590/S2237-96222025v34e20240027.en. Available at: https://doi.org/10.1590/S2237-96222025v34e20240027.en. Access in: 7 may 2026.
WORLD HEALTH ORGANIZATION. International Statistical Classification of Diseases and Related Health Problems – ICD-10: Chapter XVII – Congenital malformations, deformations and chromosomal abnormalities (Q00–Q99). Geneva: World Health Organization, 2019. Available at: https://icd.who.int/browse10/2019/en#/XVII. Accessed in: 20 may 2026.
WORLD HEALTH ORGANIZATION. International Statistical Classification of Diseases and Related Health Problems: 10th Revision. 5. ed. Geneva: World Health Organization, 2016. Available at: https://iris.who.int/handle/10665/246208. Access in: 8 may 2026.
WYSZYNSKI, Diego F.; WU, Tao. Prenatal and Perinatal Factors Associated with Isolated Oral Clefting. The Cleft Palate-Craniofacial Journal, v. 39, n. 3, p. 370–375, 2002. DOI: 10.1597/1545-1569_2002_039_0370_PAPFAW_2.0.CO_2. Available at: https://journals.sagepub.com/doi/10.1597/15451569_2002_039_0370_PAPFAW_2.0.CO_2. Access in: 10 may 2026.
XU, W. et al. Maternal Periconceptional Folic Acid Supplementation Reduced Risks of Non-Syndromic Oral Clefts in Offspring. Scientific Reports, v. 11, n. 1, p. 12316, 2021. DOI: 10.1038/s41598-021-91825-9. Available at: https://doi.org/10.1038/s41598-021-91825-9. Access in: 10 may 2026.
About the Authors
Ana Luiza M. M. F. de Souza is a PhD candidate in Genetics in the Graduate Program in Genetics - UFRJ, CNPq scholarship holder, developing the project in the area of Human Genetics at the Laboratory of Epidemiology of Congenital Malformations (IOC/FIOCRUZ) with the title: integrated and innovative analysis of Oral Clefts. Master's degree in Genetics (PGGen - UFRJ) and Bachelor's degree in Biology with emphasis on Genetics (UFRJ).
Ana Clara R. M. Gomes is graduated in Biological Sciences (Teaching Licentiate) from the Federal University of Rio de Janeiro (UFRJ). Served as a Scientific Initiation scholarship holder (PIBIC) at the Oswaldo Cruz Foundation (Fiocruz), at the Laboratory of Epidemiology of Congenital Malformations (LEMC/IOC), from August 2021 to February 2023, developing a project on the genetics of orofacial clefts. She completed her stricto sensu Master's degree in the Graduate Program in Cellular and Molecular Biology of the Oswaldo Cruz Institute (PGBCM IOC/Fiocruz), with a project also focused on the genetics of orofacial clefts, linked to the Laboratory of Epidemiology of Congenital Malformations (IOC/FIOCRUZ). Currently, she is pursuing a stricto sensu Doctoral degree in the same program (PGBCM IOC/Fiocruz). Her projects continue in the area of genetics of orofacial clefts.
Luiz Felipe R. de Souza is graduated in Biological Sciences - Genetics modality from the Federal University of Rio de Janeiro (UFRJ) and is currently a Master's student in the Graduate Program in Genetics at UFRJ, working at the Laboratory of Epidemiology of Congenital Malformations - LEMC (Oswaldo Cruz Institute/FIOCRUZ) on a project focused on the genetic and subphenotype analysis of orofacial clefts in Brazilian families treated at reference treatment centers in Rio de Janeiro.
Maria Clara B. F. de Franca is an undergraduate student in Pharmacy at the State University of Rio de Janeiro (UERJ). Clinical Analysis Technician graduated from the Joaquim Venâncio Polytechnic School of Health (EPSJV/Fiocruz). Worked as an intern at the Covid-19 Diagnostic Support Unit (UNADIG - Fiocruz) from June to September 2023, and at the Laboratory of Diagnosis, Teaching and Research of the Sérgio Arouca National School of Public Health (LADEP - ENSP/Fiocruz), from September to December 2023. Currently, since March 2025, she is a technological initiation student at the Laboratory of Epidemiology of Congenital Malformations (LEMC/IOC) at the Oswaldo Cruz Foundation (Fiocruz), focusing on genetic studies of oral clefts.
Rafaela C. N. Mattos is an undergraduate student in Biomedicine at the Federal University of the State of Rio de Janeiro (UNIRIO). Currently, she develops scientific initiation activities at the Laboratory of Epidemiology of Congenital Malformations (LEMC/IOC) at the Oswaldo Cruz Foundation (Fiocruz), mainly working on the investigation of genetic variants associated with oral clefts.
Flávia M. de Carvalho is a public health researcher at the Oswaldo Cruz Institute (Fiocruz), with a solid academic and scientific background in human and medical genetics, epidemiology, and craniofacial anomalies. Holds a degree in Dentistry and a specialization in Periodontics from UERJ, where she also completed her Master's and PhD, including a sandwich internship at the University of Pittsburgh (USA) with a focus on molecular biology. She holds a post-doctorate in Human and Medical Genetics from UFRJ, with research aimed at identifying candidate genes for oral clefts in Latin American populations. Since 2014, she has been leading projects at the Laboratory of Epidemiology of Congenital Malformations (LEMC/IOC/Fiocruz), working on population studies, applied genomics, oral cleft subphenotypes, dental anomalies, and systemic conditions impacting oral health, in addition to innovation in craniofacial photogrammetry. She has been part of the ECLAMC Network and Association since 2010, is a professor and discipline coordinator in the graduate program in Genetics at UFRJ, and a member of the Research Ethics Committee of IOC/Fiocruz. Author of publications in international journals, she collaborates in scientific networks and supervises research aimed at the genetic understanding and prevention of congenital malformations. She is currently a member of the Collegiate of the Latin American Collaborative Study of Congenital Malformations (ECLAMC).
Author Contributions
Conceptualization [A.L.M.M.F.S, A.C.R.M.G, F.M.C]; methodology [A.L.M.M.F.S, A.C.R.M.G, F.M.C]; formal analysis [A.L.M.M.F.S, A.C.R.M.G]; investigation [insert initials]; resources [F.M.C]; data curation [A.L.M.M.F.S, A.C.R.M.G]; writing, original draft, [A.L.M.M.F.S, A.C.R.M.G, L.F.R.S, M.C.B.F.F, R.C.N.M]; writing, review and editing [F.M.C]; visualization [A.L.M.M.F.S, A.C.R.M.G]; supervision, [F.M.C]; project administration, [F.M.C]. All authors read and agreed to the published version of the manuscript.
Acknowledgments
The authors thank the Health Applied Data Science Platform (PCDaS) of the Oswaldo Cruz Foundation for the organization and provision of SINASC data.
Funding
This research was funded by the National Council for Scientific and Technological Development (CNPq) 142391/2025-5 [A.L.M.M.F.S], 194895/2025-4 (M.C.B.F.F) and 173383/2025-4 [R.C.N.M] and the Coordination for the Improvement of Higher Education Personnel (CAPES) 88887.239340/2025-00 [A.C.R.M.G.], 88887.271635/2026–00 [L.F.R.S.]
Conflicts of Interest
The author declares no conflict of interest.
About Coleção Estudos Cariocas
Coleção Estudos Cariocas (ISSN 1984-7203) is a publication dedicated to studies and research on the Municipality of Rio de Janeiro, affiliated with the Pereira Passos Institute (IPP) of the Rio de Janeiro City Hall.
Its objective is to disseminate technical and scientific production on topics related to the city of Rio de Janeiro, as well as its metropolitan connections and its role in regional, national, and international contexts. The collection is open to all researchers (whether municipal employees or not) and covers a wide range of fields — provided they partially or fully address the spatial scope of the city of Rio de Janeiro.
Articles must also align with the Institute’s objectives, which are:
- to promote and coordinate public intervention in the city’s urban space;
- to provide and integrate the activities of the city’s geographic, cartographic, monographic, and statistical information systems;
- to support the establishment of basic guidelines for the city’s socioeconomic development.
Special emphasis will be given to the articulation of the articles with the city's economic development proposal. Thus, it is expected that the multidisciplinary articles submitted to the journal will address the urban development needs of Rio de Janeiro.